Download
1 / 30
310 likes | 637 Views
Mitral regurge. Prof. Lotfy Hamed Abo dahab . Professor Of Internal Medicine. Faculty Of Medicine Sohag University.

E N D
Mitral regurge Prof. LotfyHamedAbodahab. Professor Of Internal Medicine. Faculty Of Medicine Sohag University.
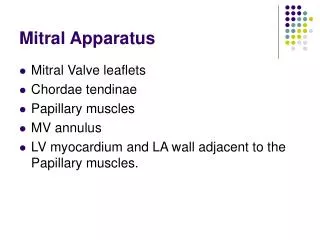
Mitral regurgeProper closure of the MV depends on: -Normal leaflets,-Normal CT to keep the leaflet in place, -Normal contractile papillary muscles to pull down the valve cusps during systole and prevent their displacement into the atrium-Normal size of the MV ring.
-Etiology of MR:.MR can result from diseases involving any of the different components of the MV as:.1-Mitral valve prolapse2-Rheumatic fever3-Dilatation of the MV ring as in HF.4-Dysfunction of the MV leaflets due to ischemia, infarction,.5-Connective tissue disease6-Annular calcifications7-Congenital cardiac conditions8-Acute mitral regurgitation (infective endocarditis – myxomatous degeneration – truma – acute myocardial infarction)9-Weight loss agents as: dexfenfluramine – fenfluramine & fenteramine
Effects:.1-LA is dilated and its pressure rises due to regurgitation of blood from LV into LA each systole.2-During diastole the large amount of blood in the LA flows to the LV across a nonstenotic MV producing turbulence of blood flow and relative MS.3-LV is dilated due to volume overload.4-LV failure lead to pulmonary congestion, HTN5-AF may occurClinical Picture:.Symptoms:.1-Mild to moderate MR is asymptomatic.2-When LV failure occurs, symptoms of pulmonary congestion appear.3-Symptoms of pulmonary HTN.
Signs:.1-LV volume overload causes:. -Hyperdynamic apex beat (displaced outward and downward).2-Regurgitation through MV causes:. -Systolic thrill at the apex. -Pan systolic murmur, propagating to the axilla. -Faint 1st HS due to (In diastole, the MV floats on the top of blood filling the LV. When systole starts the valve is already semi closed)3-Rapid flow of blood across the MV in diastole causes:. -3rd HS -Mid diastolic murmur.
* Acute mitral regurge:.Mechanism:. 1-Papillary muscle dysfunction, or rupture complicating AMI.2-MV perforation in infective endocarditis.3-Ruture CT in MVP (myxomatous degeneration).The degree and symptoms of pulmonary congestion are much greater than in chronic MR. This is because LV contraction forces the regurgitant blood into non-compliant LA still of normal size. Acute pulmonary edema may develop, and shock may develop. These patients may need urgent surgical correction.
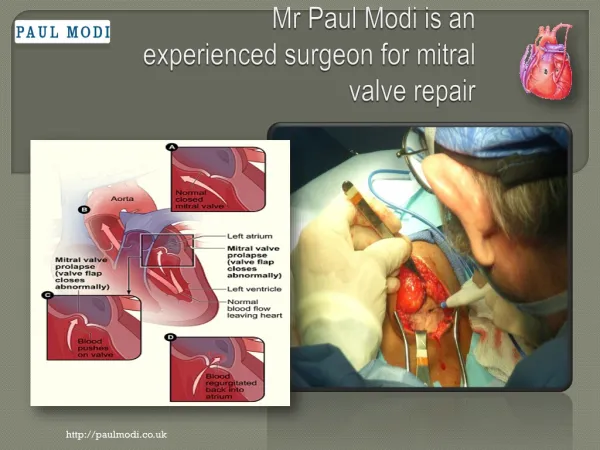
*Mitral valve prolapse:.- Prolapse of the redundant MV leaflets into the LA may occur in 10% of normal population.-Causes:. 1-Unknown 2-Marfan syndrome 3-Congenital anomaly (either isolated MVP, or in association with ASD). 4-Myxomatous degeneration of the MV.-MR may develop.-Non-specific chest pain and palpitation due to recurrent arrhythmia (usually respond to Beta blockers).-By auscultation: mid systolic click and may be late systolic murmur due to MR (click murmur syndrome).
Investigation to MR:.1-X-ray picture:.1-LA enlargement 2-LV enlargement3-Pulmonary congestion & HTN
3-Echocardiograhy:. -Degree of LV, and LA dilation -Degree of MR -PH
DifferentialDiagnosis:.1-TR 2-VSDComplications:.1-LV failure, PH and RV failure. 2-AF. 3-Thrombi in the LA may lead to systemic embolization 4-Thrombosis in the RA may also occur and result in pulmonary embolism 5-Infective endocarditis 6-Calcification of the MV 7-Recurrence of rheumatic activity
Treatment:.1-Prophylaxis against RF 2-Prophylaxis against IE. 3-Treat complications as HF, arrhythmias. 4-Afterload reducing agent as: Nitrates & vasodilators 5- ACE inhibitors (decrease the LV size) 6-Regular follow up of all patients , clinically and by Echo. *Asymptomatic patients with stable LV dimensions can be treated medically. *Symptomatic patients, severe MR ,and evidence of progressive LV dilatation Surgery must be advised before impairment of LV function. * MV repair * MV replacement.