Download
1 / 41
410 likes | 541 Views
Problem drug use, HIV and injecting: an overview of the European experience. Paul Griffiths, EMCDDA Drug Control in the Baltic Region, Vilnius, 27 September 2005. Outline of this presentation. The EMCDDA structure working methods Overview of available European data on

E N D
Problem drug use, HIV and injecting: an overview of the European experience Paul Griffiths, EMCDDA Drug Control in the Baltic Region, Vilnius, 27 September 2005
Outline of this presentation • The EMCDDA • structure • working methods • Overview of available European data on • problem drug use, • on responses to problem drug use • making special reference to injecting and HIV • A few thoughts on: • future face of problem drug use in Europe • what are some key information needs and deficits
European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) • The Central reference point for drug information in the EU • Established in 1993, based in Lisbon, Portugal • A decentralised agency of the European Union • a response to the need to cope with new tasks of a technical and/or scientific nature • agencies of particular relevance to public health; • EMCDDA – European Monitoring Center for Drugs and Drug Addiction, Lisbon (Portugal) • EMEA – European Medicines Agency, London (United Kingdom) • ECDC – European Centre for Disease Prevention and Control, Solna (Sweden)
Overview of our data collection approach • Network of national focal points in MS (REITOX ) • Annual reporting • National overview • Standard tables • Structured questionnaires • Expert groups per indicator area that meet annually • Liaison with other specialist information providers • Emphasis on encouraging adoption of common methods & in providing European level added value
EMCDDA – membership • Membership pre-2004 – the 15 EU Member States • Norway started providing data in 2001 (15+1) • May 2004, enlargement – 10 new members • Cyprus, Czech Republic, Estonia, Latvia, Lithuania, Hungary, Malta, Poland, Slovenia, Slovakia. • Candidate countries – Bulgaria, Romania and Turkey • Important to note that in some areas the new countries change… • analysis of the European situation • analysis of data availability
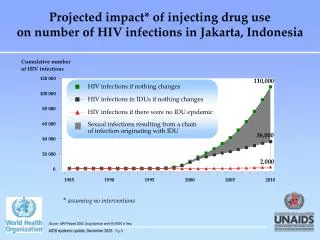
HIV and the European picture • HIV has to a large extent been one of the major issues to shape modern European drug policy • Inextricably linked with epidemic of injecting heroin use that Europe experienced over the 1990s • Stimulated investment in new methods to assess problem drug use and risk behaviours • Profoundly altered the way services were structured and orientated…. more proactive, broader set outcome objectives
The European picture is a heterogeneous onebut with some common elements • Diversity exists in respect to HIV among IDUs • Estimates of between 850,000 and 1.3 million IDUs in EU 25 • Some countries have had only small outbreaks of HIV infection and have managed to maintain very low prevalence rates • Some countries have had major epidemics ….but the overall picture now appears stable or falling in most countries • Diversity of responses • Balance of prevention, treatment and harm reduction interventions • Scale of responses & timing of responses • No simple relationship between policy and the situation • Common elements • Although major differences remain in emphasis EU members states appear now to operate within a broad policy consensus • Cautious optimism about stable or an improving situation in respect to drug injecting, HIV infections among IDUs and heroin consumption in many MS
Data sources on HIV-AIDS in IDU • Reporting from routine surveillance and HIV/AIDS case reporting (EuroHIV) • Data from EMCDDA drug related infectious disease indicator (IFD) • routine testing at drug treatment centres • studies of IDU (in and out of treatment) • Neither source provides comprehensive coverage or easily allows the monitoring of trends over time • Data set is improving
Data sources on HIV-AIDS in IDU • Routine surveillance suggests IDU no longer the main route of transmission for AIDS …but how do we interpret this? • Data weaker from routine disease surveillance for HIV prevalence in IDUs • IFD indicator suggests large differences in HIV prevalence between countries and large differences between different populations within countries
HIV prevalence among IDUs in the EU EMCDDA 2004Notes: Colour indicates midpointsLocal data shown in ()
HIV seroprevalence and diagnostic testing studies of IDUs (treatment & non treatment)
HIV in IDUs in Europe • Marked difference between countries and within some countries • High prevalence countries (old MS) Italy, Spain, Portugal, followed by France • Some high prevalence estimates from new MS (Latvia, Estonia), and worries about others (Poland) • Low prevalence countries in both old and new MS including countries with high prevalence IDU • Cautious assessment is the long term trend appears to be stable or downwards • Some small increases in recent data in some countries or in specific subpopulations • Data quality problems so analysis must be made with caution
A note on HCV prevalence in IDUs • Prevalence estimates higher and more convergent than for HIV • Clear need to finding effective prevention strategies • Routine disease surveillance sources of limited value • Drug injecting principle route of transmission for HCV in Europe
What is happening to heroin use and injecting heroin use ? • Data from… • Problem drug use indicator • Treatment demand indicator (TDI) • Drug related deaths indicator… • major cause death among young males in Europe • and among IDUs the major cause mortality • e.g. 2001 EU15 reported… 8,347 DRD as compared to 1,633 AIDS deaths among IDUs
Prevalence of problem drug use (indicator) • Operational definition PDU: “injecting, long-term or regular use of opiates, cocaine and/or amphetamines • Estimates 1.2 and 2.1 million PDUs in EU 25 • Historically mainly reflected heroin use and injecting • Amphetamines in some countries (mainly Nordic countries) • Growing heroin smoking population (from late 1980s) • Prevalence estimates produced from different sources and methods, both national and local studies (CRC, multipliers, synthetic estimation techniques) • Recently some limited work on incidence modelling mostly based on statistical inference from treatment populations • Estimates more often local. Getting national coverage more difficult • IDU estimates are particularly lacking
Estimated rate of problem drug use(1999-2003 rate per 1 000 aged 15-64)
Trend in new treatment demands (%) by drug type Data from 11 EU countries + Bulgaria from 1996 to 2003 Heroin 80 Cocaine Cannabis 70 Other Stimulants 60 50 % 40 30 20 10 0 1996 1997 1998 1999 2000 2001 2002 2003 (n.52890) (n.50844) (n.54374) (n.56407) (n.54428) (n.58007) (n.62342) (n.65336)
100 90 80 70 60 50 40 30 20 10 0 Latvia Total Malta Greece Cyprus Finland Sweden Bulgaria Slovenia Slovakia Germany Denmark Netherlands Czech Republic United Kingdom Proportion of new outpatient clients injecting opiates (2003)
Long term trend in acute drug-related deaths (1985-2003) 300 250 200 Index % (1985=100%) 150 100 50 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003* 100,0 104,5 118,7 136,9 153,7 181,0 216,4 223,5 201,8 212,2 225,4 252,4 230,1 235,6 241,1 255,4 240,1 205,8 194,9 INDEX EU 15, 1985 to 2003 index year 1985=100
45,0 Austria Germany Ireland Italy Luxembourg The Age (Years) Netherlands 30,0 Portugal Spain Sweden UK - ONS UK - DSD 15,0 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 Trend in mean age of drug related deaths 1990-2003
General observations PDU • Mixed picture in terms PDU estimates • But indicators suggest a peak of PDU in early 1990s in most countries with a stabilisation thereafter. • Injecting appears a less popular mode administration in many countries and most new heroin users to treatment are non injectors • DRD most countries getting old and trending down • Suggesting new recruitment into drug injecting and heroin use may be down • The picture looks different for some of the NMS
Overview Responses • Data collection is less well developed in this area • Treatment data is limited • substitution treatment • specialist centres • underestimate • Increase in treatment especially substitution treatment in most EU MS • Also an Increase in some harm/risk reduction interventions, particularly NSE
Introduction of MMT & NSP, 1967 to 2001(EU, Norway and Bulgaria)
450 400 350 300 250 200 150 100 50 0 LU UK ES IE MT FR PT IT SI DK EU DE NL NO SE EL BE CZ LT FI HU BG LV PL RO + 4 Estimated number of drug users in substitution treatment in 29 European countries (2003) per 100.000 population aged 15-64
600,000 537,000 500,000 400,000 351,000 265,000 300,000 207,000 200,000 73,400 100,000 0 1993 1995 1997 2000 2003 10-year trend in the number of substitution treatment clients in Europe (EU-15)
Buprenorphine Other 20% 1% Methadone 79% Proportion of substitution drugs used in medically assisted treatment in Europe, 2003
20 10 0 Luxembour Spain UK Denmark France Ireland Finland Belgium Norway Austria Greece Sweden g 14.8 12.4 7.3 5.8 4.2 2.5 1.7 1.8 1.4 0.9 0.2 0.1 low 14.8 15.8 10.8 5.8 4.2 4.3 2.2 2.2 1.9 1.7 0.2 0.2 high Provision of Needle/Syringe Programmes (number of NSPs per 1000 estimated IDUs)
Conclusions • Data in this area are often heterogeneous and should be interpreted with caution • nonetheless data availability and quality have improved considerably • It is possible to provide some better understanding of drug use and HIV in Europe and to identify trends • Large differences between countries: PDU/IDU, HIV/HCV, and in the services available • The face of problem drug use in Europe may be changing • more poly drug use, stimulants, cocaine,… • older population heroin injectors with increased service access but likely to remain major consumers of public health resources
Responses • Dramatic increase in services • Substitution treatment and NSE generally now seen as part of a comprehensive drug demand reduction strategy (with other elements) • Although marked differences still exist between countries in terms of approach and the relative balance of services available • Nonetheless estimates now suggest somewhere between a quarter and one half of those with opiate problems now receiving substitution treatment
Policy context • Data has influenced MS and stimulated resource investment • More policy consensus on the need for comprehensive package of responses including risk reduction interventions, • EU recommendation on the prevention and reduction of health-related harm associated with drug dependence (2003/488/EC) • Measures in the new European Strategy & Drug Action Plan • Better understand effective prevention HIV and HCV • Look at protective factors in low prevalence countries • General support for better monitoring across the board • Increasingly a policy culture of monitoring an assessment and thus more pressure to provide robust data
Data needs for European level monitoring • Improved monitoring of HIV in IDU populations especially targeting high risk populations • More MS providing problem drug use estimates and better strategies to get national estimates or to better understand the available local data • More estimates of IDU in particular • More work on incidence estimation • Better and more comprehensive data on capacity of the treatment system • HCV prevention? • Studies of HIV risk behaviour among NON injecting drug users likely become increasingly important
Thanks…Lucas Wiessing & Dagmar Hedrich www.emcdda.eu.int