Download
1 / 77
950 likes | 3.7k Views
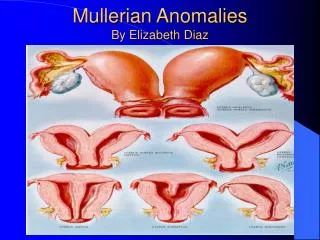
Mullerian Anomalies By Elizabeth Diaz. Mullerian Anomalies. Introduction Embryology and Development Anomalies of the Female Ductal System Clinical Presentation, Diagnosis and Treatment. Introduction.

E N D
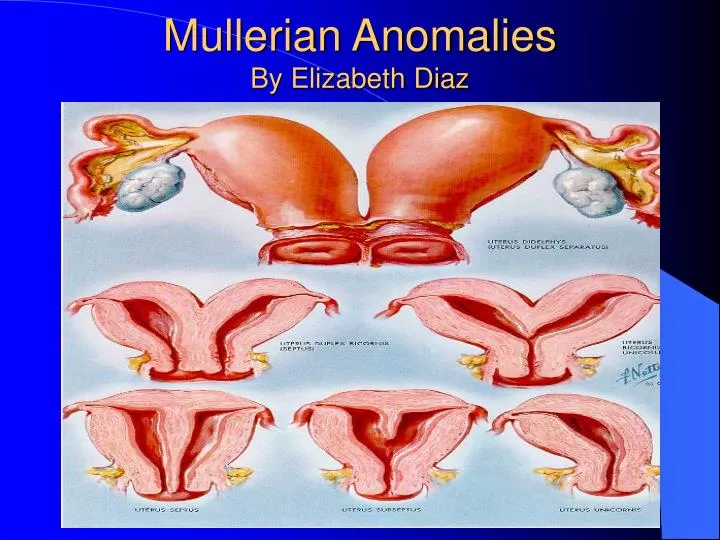
Mullerian Anomalies • Introduction • Embryology and Development • Anomalies of the Female Ductal System • Clinical Presentation, Diagnosis and Treatment
Introduction • Congenital uterine anomalies are more common than generally recognized by many practicing clinicians. • Prevalence in general population 1 in 201 (0.5%) • According to “Acien,” 2-3% of fertile women and 3% of infertile women and 5-10% of those with repeated miscarriages. • Distribution: 7% arcuate, 34% septate, 39% bicornuate, 11% didelphic, 5% unicornuate, 4% hypoplastic/asplastic/solid and other forms
Introduction • True incidence and prevalence are difficult to assess. Why? • Selection bias: 0.4% nonobstetric, 8-10% recurrent pregnancy loss. • Nonstandardized classification systems • Differences in diagnostic data acquisition resulted in widely disparate estimates • Overall prevalence; normal fertility/infertility 1% and repeated pregnancy loss 3%.
Why is this important? • Majority have no problem conceiving, but have higher rates of: • 1. Spontaneous Abortion • 2. Premature Delivery • 3. Infertility • 4. Abnormal Fetal Lie • 5. Dystocia at delivery • 6. Dysmenorrhea, endometriosis • 7. Cervical incompetence
Indifferent Embryo • Genotype of embryo 46XX or 46XY is established at fertilization • Weeks 1-6 sexually indifferent or undifferentiated stage; that is genetically female and male embryos are phenotypically indistinguishable • Week 7 begins phenotypic sexual differentiation • Week 12 female or male characteristics of external genitalia can be recognized • Week 20 phenotypic differentiation is complete.
Indifferent Embryo • Components which form the adult female and male reproductive systems are: 1. Gonads ovaries or testes 2. Genital Duct Systems Paramesonephric and Mesonephric Ducts 3. External Genitalia
5th week of pregnancy Swellings on either side of the dorsal mesentery Intermediate mesoderm forms the urogenital ridge. Gonad develops from somatic and germ cells. Somatic cells derived from mesonephric cells Formation and Differentitation of the Gonads
Coelomic epithelium and underlying mesoderm of the urogenital ridge proliferate to form the gonadal ridge Germ cells arrive in gonadal region, stimulate coelomic epithelium and mesonephros to form primitive sex cords Formation and Differentiation of Gonads
Primary sex cords develop from the gonadal ridge and incorporate primordial germ cells (XX or XY genotype) which migrate into the gonad from the wall of the yolk sac. Sex cords and germ cells essential for normal development Gonad
Y c’some: TDF ( testis determing factor), SRY (sex determining region), crucial for differentiation Primary sex cords form seminiferous cords, tubuli recti, and rete testes. Somatic cells of primary sex cords form sertoli cells and germ cells form spermatogonia Seminiferous cords: spermatogonia and sertoli cells, which secrete Anti-Mullerian Hormone (AMH) or MIS, and ABP (androgen binding protein). Mesoderm b/w seminiferous cords gives rise to Leydig cells, which secrete testosterone. Leydig cells have receptors for HCG, induced by HY antigen. Development of Testes
Development of Testes • Genital ridge SRY Testes • Primitive sex cords sertoli cells seminiferous cords • Seminiferous cords separated from superficial epithelium by tunica albuguinea • Seminiferous cords seminiferous tubules • Sertoli cells AMH/MIS • AMH ipsilateral paramesonephric regress • Leydig cell testosterone virilization wolffian duct epididymis, vas deferens, seminal vesicle.
Primary sex cords develop into the rete ovarii, which degenerate. Secondary sex cords develop and incorporate primordial germ cells Secondary sex cords break apart and form primordial follicles, which contain primary oocytes surrounded by a layer of follicular (granulosa) cells. Primary oocyte stage maintained until adulthood Formation of the Ovary
+ TDF medullary sex cords differentiate into Sertoli Cells Sertoli cells produce anti-mullerian hormone - TDF cortical sex cords differentiate into oocytes and follicular cells Lack of sertoli cells no AMH Genetic males have testis determining factor on the sex determining region SRY of the Y chromosome. Genetic males produce Testis Determing Factor in the sex cords
6th week, two pairs of genital ducts. Mesonephric Duct extending from the mesonephros (Wolff’s body) to the cloaca (urogenital sinus) referred to as the Wolffian system Second duct arises as a longitudinal invagination of coelomic epithelium on the anterolateral surface of the urogenital ridge, known as Paramesonephric or Mullerian Duct. Genital Duct Development
Cranial uterine tubes Caudal portions fuse and form the uterovaginal primordium and bring together two peritoneal folds, the broad ligament. Initially they remain separated by a septum but later they fuse to form the uterus. Paramesonephric Duct
Paramesonephric ducts do not make contact with the urogenital sinus. Paramesonephric ducts fuse with the medial wall of the mesonephric ducts. Below the caudal tip of the uterine primordium and above the dorsal wall of the urogenital sinus, with the mesoneprhic ducts lying laterally, a collection of paramesonephric cells forms constituting the Mullerian tubercle. Paramesonephric Duct
Ureteral Buds:Mesonephric ducts open caudally in urogenital sinus. At caudal tip ureteral bud sprouts. Grows laterally, anteriorly and cranially becomes metanephros to form the definitive kidney
Testis forms, the testosterone produced by leydig cells and is carried along the tubules by ABP stimulates the development of the mesonephric ducts to form the efferent ductules, epididymis, ductus deferens, and seminal vesicles. The AMH produced in Sertoli cells inhibits paramesonephric duct development. Male Genital Duct Formation
In ovary the absence of testosterone inhibits the development of the mesonephric ducts. The atretic remains form the epoophoron, paraoophoron and Gartner’s ducts. In absence of AMH, paramesonephric ducts form the female internal genital tract. Female Genital Duct Formation
Embryology of Vagina • Embryology controversial • Derived paramesonephric ducts vs. mesonephric ducts vs. urogenital sinus, or a combination. • Most accepted, superior part derived fusion paramesonephric , while inferior part arises from urogenital sinus, BUT assumes the “inductor” function of the mesonephric ducts stimulate adequate mullerian/paramesonephric development.
Mullerian tubercle cellular condensation b/w inferior part of fused paramesonephric ducts and urogenital sinus. Sinovaginal bulbs develop, constitute vaginal plate. Cavity formed lined with paramesonephric epithelium, opens into the urogenital sinus and the metaplastic induction to polystratified plain epiithelium would produce the vagina. Theory of Mullerian Tubercle.
Studies show sinovaginal bulbs are caudal segments of mesonephric ducts. Between these bulbs and caudally to the paramesonephric ducts, a solid epithelial structure is located contacting the dorsal wall of the urogenital sinus…the mullerian tubercle. Inductor role of mesoneprhic duct on vagina
Vagina derived from fused mesonephric ducts and Mullerian tubercle. Paramesonephric ducts form uterus to external cervical os and adequate formation is induced by mesonephric ducts. Mesonephric ducts regress cranially but at cervical os, they enlarge and form the sinovaginal bulbs. The paramesonephric cellular condensation (mullerian tubercle ) incorporates itself in the vaginal plate formed by fusion of the two bulbs. Cavitation allows the paramesonephric cells to line the primitive vaginal cavity with paramesonephric epithelium. Mesonephric duct induction
As ureteral bud sprouts from the opening of the mesonephric ducts in the urogenital sinus, the absence or distal agenesis of a mesonephric duct would result in an absence of its opening to the sinus ( the origin of the blind vagina) and in an absence of the ureteral bud on that side. Thus, the definitive kidney would fail to develop (ipsilateral renal agenesis) Agenesis of mesonephric duct
Development external genitalia • Early, similar in both sexes • 6th wk, three external protuberance surround cloacal membrane, the left and right genital swellings meet anteriorly to form the genital tubercle. • 12th wk identify difference. • Genital swelling labioscrotal folds scrotum or labia major • Genital tubercle phallus penis or clitoris
Role of Dihydrotestosterone • Differentiation depends indirectly on gonadal secretion in male fetus. • Testosterone acts locally on the tubules but not directly on the external genitalia. • Hormonal action is exerted by dihydotestsoterone (DHT) formed from testosterone by the 5 alpha reductase enzyme. • DHT causes external genitalia to become a penis and scrotum and induces development of prostate
Classification into 3 groups: Based on similar embryonic development defects and clinical presentation • 1. Agenesis of uterus/vagina: Rokitansky-Kuster-Hauser Syndrome. • 2. Defects in Vertical Fusion (obstructive or non-obstructive) • 3. Lateral Fusion defects (obstructive or non-obstructive).
Revised Classification System • “Acien” proposed embryological classification. • 1.Agenesis of urogential ridge absence kidney, ovary, fallopian tube, hemiuterus, hemivagina. • 2. Isolated Mullerian anomalies (probably also induced by minor mesonephric defect) affect: • A. Paramesonephric uterine and/or tubal anomalies • B. Mullerian tubercle agenesis or atresia vagina. • C. All Paramesonephric derivatives Rokitansky-Kuster-Hauser syndrome. 3. Anomalies urogenital sinus urogenital membrane (imperforate hymen).
Revised Classification System • 4. Mesonephric anomalies, with absence opening in urogenital sinus and forming ureteral bud. Usually uterine anomaly, b/c lack of inductor function of mesonephric duct, as well as unilateral renal agenesis and ipsilateral blind vagina • 5. Combination of above malformations
RKH Syndrome: Diagnosis • Expected Menarche • Difficult to differentiate from imperforate hymen • No uterus on exam, U/S, MRI, Laparoscopy, IVP • Confused with Androgen Resistance Syndrome with shallow pouch and no uterus. • Determine karyotype.
RKH Syndrome: Etiology • Molecular mechanisms for differential development: Hox-9, 10, 11, 13 are expressed along the length of mullerian ducts. Alteration of HOX genes may give rise to mullerian anomalies
RKH Syndrome: Treatment • Goal is to restore normal sexual function through creation of neovagina. • Nonsurgical: • 1. Frank technique: Pressure to perineal dimple. • 2. Ingram method: Bicycle seat stool. Surgical: Create neovagina 1. McIndoe operation: Skin graft between rectum/bladder 2. Sigmoid vaginoplasty: 3. Vecchietti operation: transabdominal approach.
Vertical Fusion Defects: obstructive and non-obstructive • Incomplete cavitation of the vaginal plate formed by the down-growing mullerian ducts and the up-growing urogenital sinus. Can be considered in two categories: • 1.Imperforate Hymen • 2.Transverse Vaginal Septum