Download
1 / 1
10 likes | 111 Views
Alcohol Abuse Characteristics of Individuals with Co-occurring Psychiatric and Substance Abuse Disorders Laurel Mangrum, Ph.D. & Richard Spence, Ph.D University of Texas at Austin, Addiction Research Institute. Affective Disorders. Schizophrenia. Introduction.

E N D
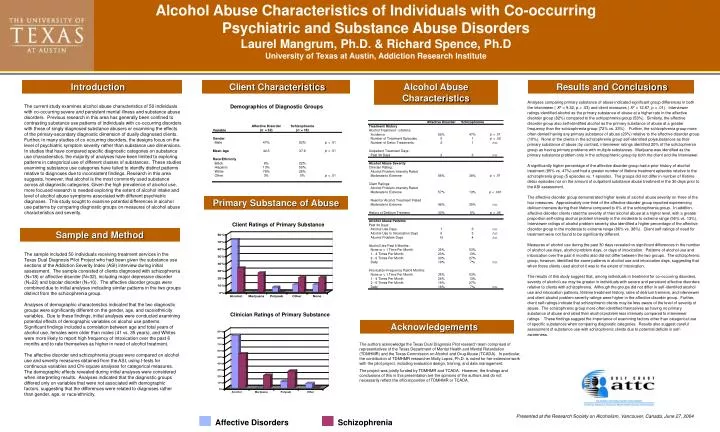
Alcohol Abuse Characteristics of Individuals with Co-occurring Psychiatric and Substance Abuse Disorders Laurel Mangrum, Ph.D. & Richard Spence, Ph.D University of Texas at Austin, Addiction Research Institute Affective Disorders Schizophrenia Introduction Client Characteristics Alcohol Abuse Characteristics Results and Conclusions • Analyses comparing primary substance of abuse indicated significant group differences in both the interviewer ( X2 = 9.32, p < .03) and client measures ( X2 = 12.67, p < .01). Interviewer ratings identified alcohol as the primary substance of abuse at a higher rate in the affective disorder group (82%) compared to the schizophrenia group (53%). Similarly, the affective disorder group also self-identified alcohol as the primary substance of abuse at a greater frequency than the schizophrenia group (72% vs. 33%). Further, the schizophrenia group more often denied having any primary substance of abuse (20%) relative to the affective disorder group (10%). None of the clients in the schizophrenia group self-identified polysubstances as their primary substance of abuse; by contrast, interviewer ratings identified 20% of the schizophrenia group as having primary problems with multiple substances. Marijuana was identified as the primary substance problem only in the schizophrenic group by both the client and the interviewer. • A significantly higher percentage of the affective disorder group had a prior history of alcohol treatment (85% vs. 47%) and had a greater number of lifetime treatment episodes relative to the schizophrenia group (5 episodes vs. 1 episode). The groups did not differ in number of lifetime detox episodes nor on the amount of outpatient substance abuse treatment in the 30 days prior to the ASI assessment. • The affective disorder group demonstrated higher levels of alcohol abuse severity on three of the four measures. Approximately one-third of the affective disorder group reported experiencing delirium tremens during their lifetime compared to 6% of the schizophrenia group. In addition, affective disorder clients rated the severity of their alcohol abuse at a higher level, with a greater proportion self-rating alcohol problem intensity in the moderate to extreme range (56% vs. 13%). Interviewer ratings of alcohol problem severity also identified a higher percentage of the affective disorder group in the moderate to extreme range (86% vs. 38%). Client self-ratings of need for treatment were not found to be significantly different. • Measures of alcohol use during the past 30 days revealed no significant differences in the number of alcohol use days, alcohol problem days, or days of intoxication. Patterns of alcohol use and intoxication over the past 6 months also did not differ between the two groups. The schizophrenic group, however, identified the same patterns in alcohol use and intoxication days, suggesting that when these clients used alcohol it was to the extent of intoxication. • The results of this study suggest that, among individuals in treatment for co-occurring disorders, severity of alcohol use may be greater in individuals with severe and persistent affective disorders relative to clients with schizophrenia. Although the groups did not differ in self-identified alcohol use and intoxication patterns, lifetime treatment history, rates of delirium tremens, and interviewer and client alcohol problem severity ratings were higher in the affective disorder group. Further, client self-ratings indicate that schizophrenic clients may be less aware of the level of severity of abuse. The schizophrenic group more often identified themselves as having no primary substance of abuse and rated their alcohol problem less intensely compared to interviewer ratings. These findings suggest the importance of examining factors other than categorical use of specific substances when comparing diagnostic categories. Results also suggest careful assessment of substance use with schizophrenic clients due to potential deficits in self-awareness. The current study examines alcohol abuse characteristics of 50 individuals with co-occurring severe and persistent mental illness and substance abuse disorders. Previous research in this area has generally been confined to contrasting substance use patterns of individuals with co-occurring disorders with those of singly diagnosed substance abusers or examining the effects of the primary-secondary diagnostic dimension of dually diagnosed clients. Further, in many studies of co-occurring disorders, the designs focus on the level of psychiatric symptom severity rather than substance use dimensions. In studies that have compared specific diagnostic categories on substance use characteristics, the majority of analyses have been limited to exploring patterns in categorical use of different classes of substances. These studies examining substance use categories have failed to identify distinct patterns relative to diagnoses due to inconsistent findings. Research in this area suggests, however, that alcohol is the most commonly used substance across all diagnostic categories. Given the high prevalence of alcohol use, more focused research is needed exploring the extent of alcohol intake and level of alcohol abuse symptoms associated with different psychiatric diagnoses. This study sought to examine potential differences in alcohol use patterns by comparing diagnostic groups on measures of alcohol abuse characteristics and severity. Demographics of Diagnostic Groups Primary Substance of Abuse Client Ratings of Primary Substance Sample and Method The sample included 50 individuals receiving treatment services in the Texas Dual Diagnosis Pilot Project who had been given the substance use sections of the Addiction Severity Index (ASI) interview during initial assessment. The sample consisted of clients diagnosed with schizophrenia (N=18) or affective disorder (N=32), including major depressive disorder (N=22) and bipolar disorder (N=10). The affective disorder groups were combined due to initial analyses indicating similar patterns in the two groups distinct from the schizophrenia group. Analyses of demographic characteristics indicated that the two diagnostic groups were significantly different on the gender, age, and race/ethnicity variables. Due to these findings, initial analyses were conducted examining potential effects of demographic variables on alcohol use patterns. Significant findings included a correlation between age and total years of alcohol use, females were older than males (41 vs. 35 years), and Whites were more likely to report high frequency of intoxication over the past 6 months and to rate themselves as higher in need of alcohol treatment. The affective disorder and schizophrenia groups were compared on alcohol use and severity measures obtained from the ASI, using t-tests for continuous variables and Chi-square analyses for categorical measures. The demographic effects revealed during initial analyses were considered when interpreting results. Analyses indicated that the diagnostic groups differed only on variables that were not associated with demographic factors, suggesting that the differences were related to diagnoses rather than gender, age, or race/ethnicity. Clinician Ratings of Primary Substance Acknowledgements The authors acknowledge the Texas Dual Diagnosis Pilot research team comprised of representatives of the Texas Department of Mental Health and Mental Retardation (TDMHMR) and the Texas Commission on Alcohol and Drug Abuse (TCADA). In particular, the contribution of TDMHMR researcher Molly Lopez, Ph.D. is noted for her extensive work with the pilot project, including evaluation design, training, and data management. The project was jointly funded by TDMHMR and TCADA. However, the findings and conclusions of this in this presentation are the opinions of the authors and do not necessarily reflect the official position of TDMHMR or TCADA. Presented at the Research Society on Alcoholism, Vancouver, Canada, June 27, 2004






