Download
1 / 32
320 likes | 554 Views
Contraceptive Care for Women with HIV Infection and their Partners. Kimberly McClellan, MSN, WHNP-BC, CRNP Director Women's Health AIDS Care Group, Chester PA ksv23@drexel.edu.

E N D
Contraceptive Care for Women with HIV Infection and their Partners Kimberly McClellan, MSN, WHNP-BC, CRNP Director Women's Health AIDS Care Group, Chester PA ksv23@drexel.edu
This teleconference is made possible by the Cooperative Agreement #5U65PS000815-03 from the Centers for Disease Control and Prevention Special thanks to AETC, Title X and CDC EMCT partners The views expressed by the speakers and moderators do not necessarily reflect the official polices of the Dept. of Health and Human Services nor does mention of trade names or organizations imply endorsement by the U.S. Government.
Objectives • Describe considerations for selecting appropriate contraceptive and compare options for women living with HIV • Explain specific consideration related to hormonal contraception and antiretroviral treatment • Identify issue related to hormonal contraception and HIV progression, transmission or acquisition
Benefits of Contraception for HIV-Positive Women • Prevents unintended pregnancy • Half of all pregnancies in U.S. are unintended • Allows women to plan a pregnancy that • Is well timed • Occurs in optimal health • Minimizes risks for perinatal transmission
Special Considerations Regarding HIV and Contraception • Potential drug interaction with antiretrovirals (ARVs) • Possible effects on HIV transmission • Possible effects on HIV acquisition • Possible effects on HIV progression
Typical Effectiveness of Contraception HIV-positive women generally have the same options as uninfected women
Oral contraceptives • Same medical criteria as for HIV-uninfected women if woman is NOT on ART • Drug-drug interactions are possible between ARVs and hormonal contraceptives (HCs) • HCs are metabolized by same pathways and cytochrome P450 enzymes as many PIs and NNRTIs • These interactions can cause changes in the efficacy of the ARV or contraception ACOG (2010), Gynecologic care for women with human immunodeficiency virus. Practice Bulletin #117.
Hormonal Contraception: Alternate Delivery Methods • Combined Patch is a thin plastic square worn on body • Releases estrogen and progestin through the skin • Works by preventing ovulation • Efficacy • Limited research suggests may be more effective than COCs • Decreased efficacy in women over 90 kg
Hormonal Contraception: Alternate Delivery Methods • Limited research suggests health risks and benefits are similar to COCs • Side Effects • Skin irritation or rash where patch is applied • Changes in bleeding pattern • Headaches • Nausea • Vomiting • Breast tenderness • Abdominal pain
Hormonal Contraception: Alternate Delivery Methods • Combined Vaginal Ring is placed into the vagina • Releases estrogen and progestin • Works by preventing ovulation • Efficacy • Limited research suggests may be more effective at preventing pregnancy than COCs
Alternative Delivery Methods • Limited research suggests risks and benefits similar to COCs • Side effects • Changes in bleeding pattern • Headaches • Nausea • Breast tenderness • Vaginitis • Leukorrhea/increase in Lactobacillus
Alternate Delivery Methods • These delivery methods also vulnerable to drug interactions • One small study found significant interaction between the estrogen and progestin hormones of the patch and lopinavir/ritonavir • More research needed on these delivery methods
DMPA • Injectable (IM,SQ) progestin only contraception • Given every 3 months • Works by preventing ovulation • Efficacy • 97% effective as commonly used • Over 99% effective when used as directed (3 pregnancies per 1000 women)
Contraceptive Implants • Thin rods or tubes containing a progestin hormone. • Provide effective contraception for at least 3 yrs. • Suppresses ovulation and changes cervical mucus. • Menstrual irregularities in most users.
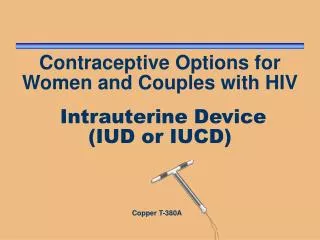
Intrauterine devices (IUDs) • No known drug interactions • No increase in shedding of HIV 2 types • Copper (Paragard) works for 10 years, may be associated with heavier menses, periods regular) • Levonorgestrel IUD (Mirena) works for 5 years, reduces menstrual blood loss (is FDA-approved as a treatment for menorrhagia), periods scant and not regular
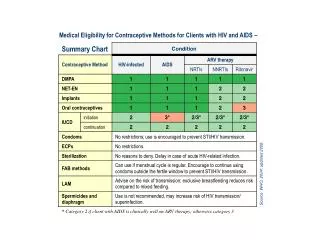
Medical Eligibility Criteria for IUD* *Adapted from: U.S. medical eligibility criteria for contraceptive use. Category 2: A condition for which the advantages of using the method generally outweigh the theoretical or proven risks. Category 3: A condition for which the theoretical or proven risks usually outweigh the advantages of using the method.
IUD and HIV Considerations • No higher risk in HIV-positive women over uninfected women for • Complications • Infections • IUD use not associated with increased risk for transmission to sex partners • Women with IUD in place who develop AIDS should be monitored for pelvic infection
Hormonal Contraception and PIs without Ritonavir Table Adapted from: Recommendations for use of antiretroviral drugs in pregnant HIV-1-infected women for maternal health and interventions to reduce perinatal HIV transmission in the United States. http://aidsinfo.nih.gov/ContentFiles/PerinatalGL.pdf
Hormonal Contraception and CCR5 antagonist/integrase inhibitor table Adapted from: Recommendations for use of antiretroviral drugs in pregnant HIV-1-infected women for maternal health and interventions to reduce perinatal HIV transmission in the United States. http://aidsinfo.nih.gov/ContentFiles/PerinatalGL.pdf
Condoms • Efficacy • Pregnancy prevention as commonly used • Male condom 85% • Female condom 79% • Pregnancy prevention when used correctly and consistently • Male condom 98% • Female condom 95% • Male condom is 80-95% effective at preventing HIV transmission when used correctly and consistently
Dual Contraceptive Use • Condom use should be encouraged for women • To prevent HIV/STI acquisition • Condom use should be encouraged in HIV-positive women • To prevent HIV transmission • Prevent STI acquisition • As an adjuvant to contraceptives • Condoms alone have a failure rate of 15%-21% at preventing pregnancy
Spermicides: Not recommended • Spermicides are not recommended by CDC • Disrupt cervical mucosa • Potentially increase viral shedding • Increase transmission of HIV to uninfected partners • Diaphragms and cervical caps are not encouraged by the CDC due to concerns about their use with spermicides
Female and Male Sterilization • Contraceptive sterilization is the most widely used method of family planning • Clients should be advised that sterilization should be considered permanent • Male-vasectomy: Cutting/occluding both vas deferens • 1st yr failure rate-0%-0.5% • Female-sterilization • Transabdominal • Transcervical • Tubal sterilization • Occlusion method
Hormonal Contraception and HIV Acquisition: WHO Technical Statement • Most studies found no statistically significant association between oral contraception and HIV acquisition • Evidence on injectable HC varied with some studies showing increases between 48% to 100% and other studies reporting no association • Due to inconsistent data and limitations of the studies performed WHO rated the current evidence as low
HIV Transmission and Hormonal Contraception: WHO Technical Statement • Recent observational study found a 2-3 increase in HIV transmission in women using injectables over oral contraception • Findings from studies assessing HC and genital HIV shedding are not consistent • Studies assessing HC and viral load generally showed no negative effect • WHO rates the evidence for HIV transmission and injectable use as low and HIV transmission and oral contraception as very low
HIV Disease Progression and Hormonal Contraception: WHO Technical Statement • None of the 10 observational studies conducted found a significant association between hormonal contraception and HIV progression • One randomized controlled trial found an increased risk of progression for HC users compared to copper IUD users • Due to flaws in this study --- high rates of method switching and loss to follow-up --- the evidence for HC and HIV progression is rated as low
WHO Recommendations • No restriction on the use of any hormonal contraceptive method for HIV-positive women or women at high risk for HIV infection • Critical importance must be placed on the consistent and correct use of condoms for the prevention of HIV acquisition or transmission • Most concern is focused on the evidence of HIV acquisition and DMPA because a causal relationship is neither established nor ruled out • Voluntary use of contraception by HIV positive women who wish to prevent pregnancy continues to be an important PMTCT strategy
Thank you! Contact the FXB Center with questions or comments, or for a copy of the slide set: Mary Jo Hoyt hoyt@umdnj.edu