Download
1 / 19
380 likes | 1.35k Views
Pyomyositis. Kunwardeep Sohal , PGY 3. What is it and Epidemiology. A purulent infection of skeletal muscle that arises from hematogenous spread, usually with abscess formation

E N D
Pyomyositis KunwardeepSohal, PGY 3
What is it and Epidemiology • A purulent infection of skeletal muscle that arises from hematogenous spread, usually with abscess formation • Classically an infection of the tropics, although it has been recognized in temperate climates with increasing frequency (most ly in adults, with males affected more than females) • Most patients with tropical pyomyositis are otherwise healthy without underlying comorbidities, while most patients in temperate regions are immunocompromised or have other serious underlying conditions
Predisposing Factors • Immunodeficiency: HIV, Diabetes, Malignancy, Cirrhosis, Renal Insufficiency, Organ Transplantation and Immunosuppressive agents • HIV particularly important; the predisposition to pyomyositis is unclear, but factors may include immune compromise, primary HIV myopathy, antiretroviral therapy, and increased rates of staphylococcal carriage • In a review of 98 cases in North America, about half of pyomyositis patients with underlying medical conditions were seropositive for HIV (Clin Infect Dis1992)
Contd • Trauma: about 25-50% of patients with pyomyositis report a history of trauma. In addition, pyomyositis has been described in temperate regions among athletes performing vigorous exercise, suggesting the potential role of minor muscle damage in the pathogenesis of the disease • Postulation? Possibly related to hematoma formation, followed by infection or increased perfusion due to trauma (making this area a favorable environment for bacteria with additional iron being provided)
Others • Injection drug use, and concurrent infection (toxocariasis-cat or dog roundworm, varicella infection)
Micro • Staphylococcus aureus is the most common cause of pyomyositis; it causes up to 90 percent of tropical cases and up to 75 percent of temperate cases (with MRSA and community acquired strains becoming the most dominant) • Group A streptococci is the second most common pathogen • Usually polymicrobial in diabetic patients
Clinical Manifestations • Hallmark: fever and pain/cramping in single muscle group • Occurs most often in lower extremities (sites include the thigh, calf and gluteal muscles) • Multifocal infection with involvement of more than one muscle group may be observed in up to 20 percent of cases
STAGES • Stage 1: crampy local muscle pain, swelling, and low-grade fever • mild leukocytosis • induration of affected muscle may be present; no fluctuation; deep abscess may not be discretely palpable, but the muscle may have a "woody" texture on palpation • 2% of patients present at this stage • Stage 2: usually 10-21 days after onset of symptoms • characterized by fever, exquisite muscle tenderness, and edema • frank abscess may be clinically apparent • marked leukocytosis • 90% present at this stage
STAGES, contd • Stage 3: systemic toxicity, affected muscle is fluctuant • Complications of S. aureusbacteremia such as septic shock, endocarditis, septic emboli, pneumonia, and ARF may be present • Course and presentation is variable with most presenting in Stage 2, however can be indolent, a delay in diagnosis in such cases may result in involvement of multiple muscle groups, requiring prolonged therapy • **Occurs as a result of bacteremia, must r/o endocarditis!
Differential Dx • Muscle strain • Contusion • Hematoma • Cellulitis • DVT • Osteomyelitis • Septic arthritis • Neoplasm • Clostridialmyonecrosisvs necrotizing fasciitis vsspontaneous gangrenous myositisvsdiabetic muscle infarction vsseptic arthritis and other forms of myositis
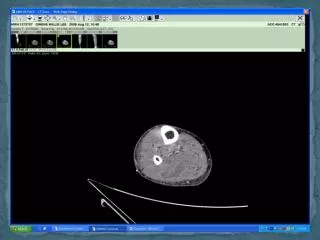
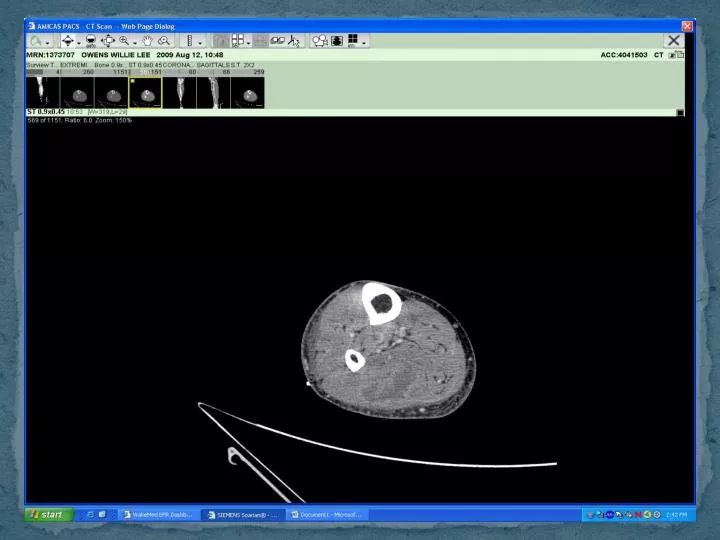
Diagnosis • Radiology, cultures and lab data • Radiology: Computed tomography (CT) is helpful for detecting muscle swelling and well-delineated areas of fluid attenuation and rim enhancement with contrast (VIR directed drainage); MRI picks up subtle differences in terms of extent in muscle • Cultures: positive in up to 10 percent of tropical cases and 35 percent of temperate cases • Lab data: leukocytosis with shift, elevated inflammatory markers (ESR, CRP), eosinophiliashould raise suspicion for a concomitant parasitic infection • **Counterintuitively, CK levels are often normal
Treatment • Although stage 1 pyomyositis can be treated with antibiotics alone, most patients present with stage 2 or 3 disease and therefore require both antibiotics and drainage for definitive management • Drainage: CT-guided percutaneous drainage is the modality of choice when feasible • However, in the setting of deep infection or extensive muscle involvement with significant necrosis, surgical intervention may be required • Diagnostic drainage can also be performed initially to direct antibiotic therapy
Treament, contd • Abx: For immunocompetent individuals, initial empiric parenteral antibiotic therapy should be directed against staphylococci and streptococci • Empiric therapy for MRSA should be initiated for patients with a previous episode of proven MRSA infection, patients with risk factors for MRSA, and patients with systemic toxicity • In addition, it should be considered in communities where the prevalence of MRSA is greater than 30 percent • For immunocompromised individuals, vancomycin may be combined with a broad spectrum regimen that has activity against gram-negatives and anaerobes
Treatment, contd • Duration: 3-4 weeks of parenteral therapy is usually sufficient, although patients with extensive, multifocal or poorly drained infection may warrant longer courses of therapy (obviously longer if endocarditis or osteo present)