Download

1 / 54
600 likes | 944 Views
Tumors of the small and large intestines. Non-neoplastic polyps Neoplastic ( epithelial) polyps Mesenchymal lesions Lymphoma. Tumors of the small and large intestine. Epithelial tumors are a major cause of morbidity and mortality worldwide

E N D
Tumors of the small and large intestines Non-neoplastic polyps Neoplastic ( epithelial) polyps Mesenchymal lesions Lymphoma
Tumors of the small and large intestine • Epithelial tumors are a major cause of morbidity and mortality worldwide • The colorectal cancer is the GIT segment most commonly affected by tumors • It is the host to more primary tumors than any other tumor of the body. • Colonic carcinoma is second to bronchogenic carcinoma as a cause of death in USA. • Adenocarcinomain colorectum represent 70% of all malignancy of GIT • Benign tumors, primarily epithelial, are present in 25 to 50% of older adults.
Terminology of Intestinal Tumors Polyps and Polyposis Syndromes • Polyp is a mucosal growth that protrude into the lumen of gut. It could be sessile or pedunculated • Polyps may be formed as the result of abnormal mucosal maturation, inflammation, or as epithelial proliferation with dysplasia
Terminology of Intestinal Tumors • Polypoid lesions is the inflammatory masses, hamartomas and tumors arising from the submucosa or muscle coat, but also protruding into the lumen. • Polyposis is multiple polyps. • Polyposis syndrome is hereditary, characterized by the presence of multiple pedunculated or sessile tumors of the mucosa
Tumors of the small and large intestineClassification • Non-neoplastic polyps • Hyperplastic polyps • Hamartomatous polyps (Juvenile & Peutz-Jeghers polyps) • Inflammatory polyps • Lymphoid polyps • Neoplastic ( epithelial) polyps • Benignpolyps (adenoma) • Malignant lesions • Adenocarcinoma • Carcinoid • Anal zone carcinoma • Mesenchymal lesions • GIT stromal tumors (benign & malignant) • Others ( lipoma, neuroma, angioma, Kaposi sarcoma) • Lymphoma
Intestinal Polyps Non-Neoplastic Polyps • Represent 90% of all epithelial polypi found in large intestine. • Found in more than half of all persons age 60 years or older. • Types: 1. Hyperplastic polyp. 2. Hamartomatous polyp (Juvenile & Peutz- Jeghers) 3. Inflammatory polyp 4. Lymphoid polyp
Intestinal Polyps 1] Hyperplastic Polyp • Asymtomatic • > 50% are located in the rectosigmoid, 20% in the ascending colon. • Smooth, moist, round, small (0.5cm) sessile lesions. • Multiple polyps are frequent. • Composed of well-formed glands and crypts lined by differentiated goblet or absorptive cells. • Pure hyperplastic polyps have no malignant potential. • Larger hyperplastic polyps; foci of adenomatous change.
Non-Neoplastic Polyp 2]Hamartomatous polyp Juvenile Polyps (retention polyp) • Developmental malformations affecting the glands and lamina propria, having no malignant potential. • commonly occur in children under 5 years old in the rectum. In adult called retention polyp. • Painless rectal bleeding after defecation. • Large, rounded, smooth lesions with a stalk • Histology: mucus-filled, cystically dilated tubules lined by normal or inflamed mucosa. • Juvenile polyposis syndrome. Occurrence of multiple hamartomatous polyps throughout the GI tract.
Non-Neoplatic Polyps 2] Hamartomatous Polyps Peutz-Jehgers polyps • Uncommon hamartomatous polyps accompanied by mucosal and cutaneous pigmentation around the lips, oral mucosa, face and genitalia. • Rare, autosomal dominant. • Caused by germ-line mutation in the LKB1 gene, which encodes a serine threonine kinase. • Polyps tend to be large and pedunculated. • May occur anywhere in the GI tract. • Have an increased risk of developing carcinoma of the pancreas, breast, lung, ovary and uterus.
Non-Neoplastic Polyps 3] Inflammatory Polyps • Occur in patients with longstanding IBD, especially in chronic ulcerative colitis. • Usually multiple. • Represent an exuberant reparative response to longstanding mucosal injury called pseudopolyps
Neoplastic Polyps (Adenomas) Adenomatous Polyp • Occur mainly in large bowel. • Prevalence: 20% to 30% before age 40, 50% after age 60. • Males and females are equally affected • Spordic and familial • Vary from small pedunculated to large sessile • Epithelium proliferation and dysplastia with loss of basal orientation of nuclei (pseudostratified). • Divided into: • Tubular adenoma has less than 25% villous architecture • Villous adenoma villous architecture over 50% • Tubulovillous adenoma villous architecture between 25 and 50%.
All adenomatous lesions arise as the result of epithelial proliferation and dysplasia, which may range from mild to so severe as to represent transformation to carcinoma.
Neoplastic Polyps 1] Tubular adenoma • Represents 75% of all neoplastic polyps. • Occurs sporadicaly and in well defined hereditary syndromes. • Average age is 60 years • 75 % occur in the distal colon and rectum. • More than 50% occur singly. • Size: few millimeters (sessile) to many centimeters (have stalk). • Stalk has a central core of fibrovascular tissue, covered with dysplastic colonic mucosa. • Severe dysplasia and invasive carcinoma may supervene.
Neoplastic Polyps 2] Villous Adenoma • The least common, largest and most ominous of epithelial polyps. • Age: 60 to 65 years, M:F ratio roughly equal. • Present with rectal bleeding or anemia, large ones may secrete copious amounts of mucoid material rich in protein. • 75% located in rectosigmoid area.
Neoplastic Polyps 2] Villous Adenoma • Morphology • Size: 1 to 10 cm in diameter. • Most are broad, sessile, velvety lesions projecting 1 to 3 cm. • Frondlike papillary projections of adenomatous epithelium with a delicate fibrovascular core. • All degree of dysplasia with frank invasive carcinoma in up to 40%.
Neoplastic Polyps 3] Tubulovillous adenoma • Intermmediate in size, frequency of having a stalk, degree of dysplasia and malignant potential between tubular and villous adenomas.
Neoplastic Polyps Clinical features • The smaller adenomas are usually asymptomatic, occult bleeding. • Villous adenomas are much more frequently symptomatic because of overt or occult rectal bleeding or mucoid material rich in protein and potassium to produce hypoproteinemia or hypokalemia. • Adenomas in the immediate vicinity of the ampulla of Vater may produce biliary obstruction.
Relationship of Neoplastic Polyps to Carcinoma • Adenoma to carcinoma sequence is documented by several observations and genetic alterations. • The probability of carcinoma occuring in a neoplastic polyp is related to: 1. The size of the polyp. 2. The relative proportion of its villous features. 3. The presence of significant cytologic atypia (dysplasia) in the neoplastic cells.
Familial Polyposis Syndrome • Patients have genetic tendencies to develop neoplastic polyps, most often autosomal dominant. Familial polyposis coli (FPC) • Genetic defect ch5 q21. • Innumerable neoplastic polyps in the colon (500 to 2500) • Polyps are also found elsewhere in alimentary tract • Most polyps are tubular adenomas • The risk of colorectal cancer is 100% by midlife. Gardener’s syndrome • Polyposis coli, multiple osteomas, epidermal cysts, and fibromatosis. Turcot syndrome • Polyposis coli, glioma and fibromatosis
Malignant Tumors of Large IntestineAdenocarcinoma • Constitutes 98% of all cancers in the large intestine. • Worldwide distribution, highest incidence in west. • Causes 15% of all cancer-related death in the USA. • The mortality rate and incidence is higher in blacks. • Peak incidence in the sixth to seventh decade.
Malignant Tumors of Large IntestineAdenocarcinoma • Predisposing factors: IBD, polyposis syndrome. • Male:female ratio is 2:1 in rectal cancer, roughly equal in colon cancer, generally males are affected about 20% more than females. • Diet appears to play an important role in the risk for colon cancer: - Low content of unabsorpable vegetable fibre. - High content of refined carbohydrates. - High fat content. - ? Increased intake of nitrites, nitrates (nitrosamines). - Reduced intake of vit A, C & E. • The use of aspirin and NSAID (cyclooxygenase-2 inhibitors) exerts a protective effect against colon cancer
When colorectal cancer is found in a young person, preexisting ulcerative colitis or one of the polyposis syndromes must be suspected. • Individuals with hereditary nonpolyposis colorectal cancer syndrome (HNPCC, also known as Lynch syndrome), caused by germ-line mutations of DNA mismatch repair genes, are at a high risk of developing colorectal cancers. • (HNPCC patients are also at risk of developing other tumors, such as cholangiocarcinomas.)
Malignant Tumors of Large IntestineAdenocarcinoma Colorectal carcinogenesis • Two pathogenetically distinct pathways for the development of colon cancer, both seem to result from accumulation of multiple mutations • The APC/B-catenin pathway • chromosomal instability that results in stepwise accumulation of mutations in a series of oncogenes and tumor suppressor genes. • Localized colon epithelial proliferation followed by the formation of small adenomas, become more dysplastic, and ultimately develop into invasive cancers.
Malignant Tumors of Large IntestineAdenocarcinoma Colorectal carcinogenesis This adenoma-carcinoma sequence accounts for aboout 80% of sporadic colorectal cancers.
Malignant Tumors of Large IntestineAdenocarcinoma The DNA mismatch repair genes pathway: • 10% to 15% of sporadic cases. • There is accumulation of mutations (as in the APC/B-catenin schema) but the involved genes are different. • Unlike in the adenoma-carcinoma sequence, there are no clearly identifiable morphologic correlates
Malignant Tumors of Large IntestineAdenocarcinoma • In DNA mismatch repair genes pathwaydefective DNA repair caused by inactivation of DNA mismatch repair genes is the fundamental and the most likely initiating event in colorectal cancers • Inherited mutations in one of five DNA mismatch repair genes (MSH2, MSH6, MLH1, PMS1, AND PMS2) give rise to the hereditary non polyposis colon carcinoma (HNPCC) • MLH1 gene is the one most commonly involved in sporadic colon carcinomas
Malignant Tumors of Large IntestineAdenocarcinoma • Microsatellite instability (MSI) is the molecular signature of defective DNA mismatch repair • Most microsatellite sequences are in noncoding regions of the genes so mutations in these genes are probably harmless. • However, some micorsatellite sequences are located in the coding or promoter region of genes involved in regulation of cell growth.
Colorectal Carcinoma Morphology • Sixty to 70% of colorectal carcinomas are in the rectum, rectosigmoid and sigmoid colon. • Left-sided carcinomas tend to be annular, encircling lesions with early symptoms of obstruction. • Neoplasms start superficially, slowly invading the deeper layers with ulceration and eventually metastasis.
Colorectal Carcinoma Morphology • Right-sided carcinomas tend to grow as polypoid, fungating masses, obstruction is uncommon. • Invasion of the wall and extend to the mesentery, regional lymph nodes and more distal sites. • Mucinous adenocarcinoma secret abundant mucin that may dissect through cleavage planes in the wall. • Small cell undifferentiated carcinomas are rare (arising from neuroendocrine cells) • In UC, poorly differentiated infiltrative adenocarcinoma without an exophytic growth.
Colorectal Carcinoma Clinical features • The condition tends to be present for a considerable time before producing symptoms. • Left-sided lesions tend to present earlier but also have a more infiltrative growth pattern and a poorer prognosis. • Right-sided lesions tend to present with weakness, malaise, weight loss, unexplained anemia (secondary to early bleeding).
Colorectal Carcinoma • Spread: - direct extension. - metastasis through: - lymphatic - blood vessels - favored sites are regional lymph node, liver, lungs, bones. • Serum levels of carcinoembryonic antigen (CEA) are related to tumor size and extent of spread. They are helpful in monitoring for recurrence of tumor after resection. • Overall 5-year survival is 35 to 49% in the United States.
Colorectal Neoplasm Other Tumors • Malignant spindle cell (mesenchymal) tumors and lymphomas. • Grossly and microscopically resemble those arising elsewhere in the GI tract. • Carcinoid tumors may arise anywhere in the colon, especially the rectum. • Squamous cell carcinomas are largely limited to the rectal canal. Initially present as plaque-like lesions, later becoming ulcerated or fungating. • Malignant melanoma at the anal verge.
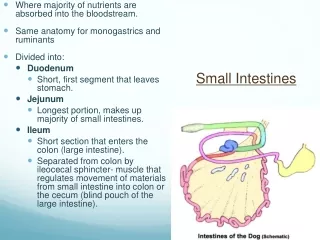
Small Intestinal Neoplasms • 3-6% of GIT neoplasm, slight preponderance to benign tumors. BENIGN • Discovered incidentally, leiomyoma, adenoma and lipoma • Large lesions may cause obstruction, bleeding, intussusception, volvulus. ADENOMAS • Single or multiple polyps, most often in the duodenum and ileum. • There is a risk of malignancy with larger adenomatous polyps. MALIGNANT • In descending order of frequency: carcinoid, adenocarcinomas, lymphomas and leiomyosarcomas. • Leiomyosarcomas have tyrosine kinase receptors, can be treated by STI-571
Small Intestinal Neoplasms Adenocarcinoma of small intestine • Tumors grow as polypoid fungating ulcerating mass or encircling pattern • Site: duodenum ( ampulla of Vater) • Presentation: abdominal cramping pain, vomiting and weight loss • Patients present late • 5 years survival is 70% after en bloc resection
Small Intestinal Neoplasms Carcinoid Tumors • Neoplasms arising from endocrine cells Kulchitsky or enterochromaffin cells found along the length of GIT mucosa. Cells have an affinity for silver salts. • 60 to 80% appendix and terminal ileum: 10 to 20% rectum, the remainder in the stomach, duodenum or esophagus. • Other Location: Lungs, pancreas, biliary tract, ovaries and liver. • Peak age: 6th decade, comprise 2% of colorectal carcinoma and 50% of small intestinal carcinoma. • Tumors in the appendix and rectum, although spreading locally, seldom metastasize. • Ileal, gastric, and colonic carcinoids are frequently malignant.
CarcinoidTumors Morphology • Round submucosal elevations that are bright yellow or yellow-gray, may be deeply infiltrative and penetrate muscle to the serosa. • Gastric and ilealcarcinoids are frequently multiple. • Tumor cells arranged in trabecular, insular, glandular or undifferentiated patterns are monotonously similar to each other with regular round nuclei • Ultrastructral features: neurosecretory electron dense bodies in the cytoplasm
Small Intestinal Neoplasms Carcinoid Tumor Clinical features • Asymptomatic • May cause obstruction, intussusception or bleeding. • May elaborate hormones: Zollinger-Ellison, Cushing’s carcinoid or other syndromes. • 5 years survival rate is 90%, small bowel Carcinoid with liver metastasis the 5 years survival rate is better than 50%
Small Intestinal Neoplasms Carcinoid tumor Carcinoid syndrome • Syndrome occur in 1% of all pt. with carcinoid & in 20% of those of widespread metastasis • Paroxymal flushing, episodes of asthma-like wheezing, right-sided heart failure, attacks of watery diarrhea, abdominal pain, edema and pellagra-like lesions of the skin and oral mucosa. • The principal chemical mediator is serotonin (5-hydroxy-tryptamine-5HT). • 5-HT is decarboxylated in the liver and lungs to 5-hydroxy-indoleacetic acid (5HIAA) • The syndrome is classically associated with ileal carcinoids with hepatic metastases.
Small Intestinal Neoplasms Lymphoma • Up to 40% of lymphomas arise in sites other than lymph nodes, gut is the most. • 1% to 4% of all gastrointestinal malignancies are lymphomas. • Primary GIT lymphomas exhibit no evidence of liver, spleen, or bone marrow involvement at the time of diagnosis.