Download
1 / 29
480 likes | 1k Views
Male Infertility Workup and Testing. Dr.Faisal Almaslami IVF Manager Al- Qassim Hospital Msc Clinical Embryology -UK American Board of Clinical Embryology ESHRE Certified Senior Clinical Embryologist. Learning Objectives. At the end of this presentation ,participant should be able to:

E N D
Male Infertility Workup and Testing Dr.Faisal Almaslami IVF Manager Al-Qassim Hospital Msc Clinical Embryology -UK American Board of Clinical Embryology ESHRE Certified Senior Clinical Embryologist
Learning Objectives At the end of this presentation ,participant should be able to: • Explain indications for male infertility workup • List commonly used tests to assess the infertile male patient. • Identify indications for more complex laboratory and diagnostic testing.
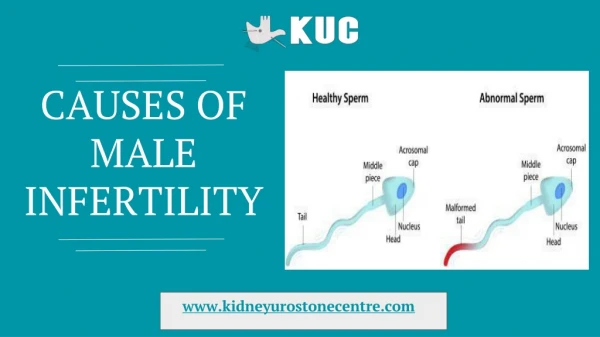
Terminology • Aspermia : no semen is present • Azoospermia : no sperm in semen • Sever oligospermia : < 5 million sperm /ml • Asthenozoospermia : reduced sperm motility • Teratozoospermia : abnormal sperm morphology
Introduction • Male factor • Sole factor in 20% of infertile couple • Contributes in another 30-40% • Variety of causes • Idiopathic-no identifiable cause • Unexplained infertility inability to conceive but no abn. found in man or women
Goals of Evaluation • Identify/treat correctible conditions • May improve male’s fertility • Allow for conception via intercourse • Identify uncorrectable conditions treatment options: • Assisted reproduction technology • Detect genetic causes of male infertility • identify potential for transmission of genetic abnormalities • Identify underlying medical conditions
Timing of male evaluation • Failure to achieve a successful pregnancy • After 12 months of unprotected intercourse • After 6 months • Based on history and physical finding • For women >35 years • Men concerned about future fertility even in absence of current partner
Initial Screening Evaluation • Reproductive history • At least one semen analysis • Men with primary or secondary infertility are evaluated in the same manner
Reproductive History • Coital frequency and timing • Duration of infertility ,prior fertility • Childhood illness and developmental history • Systemic medical illness, prior surgery • Medications and allergies • Sexual history, including STD • Gonadal toxin exposure (heat,chemical,environmental)
Semen Analysis • Cornerstone of lab. evaluation of male infertility • 2-5 days abstinence • Collection method • Collection site –keep at RT or body temp.and analyze within 1 hr.
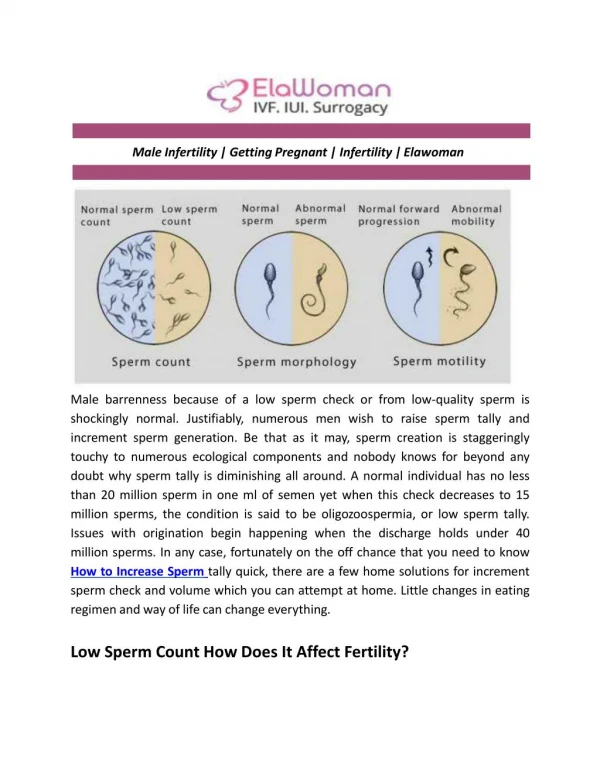
Semen Analysis • Volume,Conc,Motility,Morphology • Methods /Protocols defined by WHO • Diagnosis of AZOOSPERMIA -After centrifugation and examination of pellet • Reference value for semen are not the same as minimum values required for conception
Semen Analysis WHO 2010 reference values • Volume 1.5-6.8 ml • pH >7.2 • Concentration 15 million /ml • Total count 39 million/ejaculate • Motility 40% • Normal morphology 4%
Evaluation for Male Infertility • Indication for a thorough evaluation: • Abnormal history or semen parameter • Unexplained infertility • Infertility after successful treatment of identified female factor • Referral to a specialist in male reproduction
Medical History • Risk factors, behaviors and lifestyle choices • All factors for reproductive history • Complete medical and surgical history • Medications • Allergies • Review of systems • Family reproductive history • Past infections • Detailed social history (gonadotoxin exposure, steroids use, drugs ,alcohol ,tobacco)
Physical Examination • Penis –location of urethral meatus • Testes-palpation and measurement • Vasa and epididymes-presence and consistency • Varicocele • 2dry sex characteristics • Digital rectal exam
Endocrine Evaluation • Serum FSH • Total testosterone level • If low (< 300 ng/ml): • LH • Prolactin • Bioavailable testosterone
Post ejaculatory urinalysis • Low or absent ejaculate • Retrograde ejaculation • For men with • Ejaculation volume <1 ml • Normal hormones • Normal vasa
Ultrasonography • Transrectal US • Seminal vesicle diameter, ejaculatory duct dilation, prostate cyst • Scrotal US Varicocele Epididymal dilation Testicular tumor
Specialized tests • WBC in semen • Increase WBC is associated with poor sperm function and motility • Pyospermia (>1million leukocyte/ml) • Evaluation for genital tract infection or inflammation
Specialized tests • Antisperm antibodies testing • Indicated for isolated asthenospermia with normal concentration or sperm agglutination • Found in serum ,seminal plasma or directly bound to sperm • Form with breakdown of the blood testes barrier
Specialized tests • Sperm viability tests • Indicated when sperm motility <5% • Eosin Y & trypan blue dye tests • Hypo-osmotic swelling test(HOS) • Viable sperm with intact cell-membrane function swell when placed I hypo-osmotic solution • Sperm can be used for IVF
Specialized test • Sperm DNA fragmentation tests • DNA integrity is important for embryo development • Sperm DNA damage • More common in infertile men • May contribute to poor reproduction • No proven role for routine use in evaluation of male infertility
Genetic screening • Genetic abnormalities • Can affect sperm production or sperm transport • Increased risk of men with: • Nonobstructive azoospermia • Sever oligospermia
Genetic screening • Most common • Numeric and structural chromosomal abnormalities • Y-chromosome microdeletions • Obstructive azoospermia due to CBAVD • Abnormality of the cystic fibrosis transmembrane conductance regulator gene(CFTR)
Cystic fibrosis Gene Mutation • Strong association between CBAVD and CFTR gene mutation • All men with CBAVD are assumed to have CFTR gene mutation • Test partner to determine risk of conceiving a child with cystic fibrosis
Karyotypic Chromosomal Abnormalities • 7% of infertile men • Proportional to sperm count • <1% in men with normal sperm concentration • 5% in oligospermic men • 10-15% I azoospermic men • Two thirds have sex chromosome aneuploidy(Klinefelter syndrome)
Y-chromosome Microdeletion • 10-15% of men with azoospermia or sever oligospermia • Occur in long arm of y chromosome (Yq11)known as (AZF) • The DAZ gene is in the AZFc region
Summary • Work-up and testing is essential to identify both correctable and uncorrectable conditions • Thorough medical and reproductive history and physical examination • Semen analysis provides basis for identifying cause and planning further testing and treatment.