Download
1 / 13
150 likes | 285 Views
Pneumococcal Immunization in the Elderly. U.S. Burden of Pneumococcal Disease in the Elderly. Invasive disease (IPD = bacteremia, pneumonia with bacteremia, uncommonly meningitis) 38 / 100,000 person years Mortality = 7.2 / 100,000 persons years Disproportionate impact among Blacks

E N D
U.S. Burden of Pneumococcal Disease in the Elderly • Invasive disease (IPD = bacteremia, pneumonia with bacteremia, uncommonly meningitis) • 38 / 100,000 person years • Mortality = 7.2 / 100,000 persons years • Disproportionate impact among Blacks • Increased rate in patients with DM, cardio-pulmonary disease, solid tumors, EtOH abuse. • Community-acquired pneumonia (CAP) • 350 - 620,000 hospitalizations per year in elderly • 20-60% pneumococcal (25-30% best estimate)
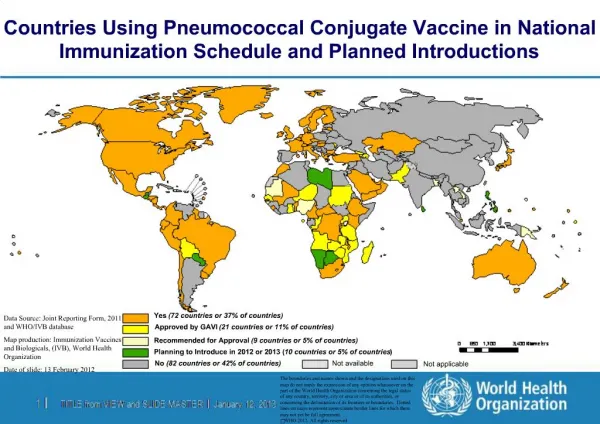
Impact of Conjugate Vaccine in the Elderly Indirect Impact on Rates of IPD in the Elderly Increasing Rate of Non-Vaccine Serotypes in Children Approval of conjugate vaccine Decreasing rate of PCN-susceptibility here ABCs Report, Emerging Infections Program Network Huang SS, et al. Pediatrics 2005; 116:e408-414
Impact of Conjugate Vaccine in the Elderly • IPD in the elderly has dropped sharply in conjugate era, but some subsets show less marked effect. • Absolute rate of pneumonias with invasive disease and non-conjugate serotypes has increased 11.6% Bacteremia/meningitis + Pneumonia in the Elderly Lexau CA, et al. JAMA 2005; 294:2043
Evidence Regarding Pneumococcal Vaccines in the Elderly • Invasive pneumococcal disease: • No compelling evidence from RCTs (low power), • Meta-analyses are heterogeneous and still underpowered, but • Observational cohort and case-control studies monotonously show 45-65% efficacy and are really the basis of current recommendations. • Community-acquired pneumonia: • No evidence from RCT • Observational studies are heterogeneous, but often (not always) are quite underpowered • Meta-analyses aren’t helpful.
Cost-Effectiveness • 23-PS vaccine is generally believed to be acceptably cost-effective in the elderly. • Multiple analyses in different countries • Typically acceptably cost-effective, in some cases cost-saving; but critically dependent on assumptions. • Earlier analyses more dramatic, but assumed efficacy against pneumococcal CAP, • More recent estimates reverse this trend and focus on IPD, but still show acceptable cost-effectiveness even considering IPD costs alone.
ID Biomedical Approach to Pneumococcal Vaccine • ID Biomedical candidate is a chimeric protein representing immunodominant and surface-exposed domains of two conserved pneumococcal proteins. • Current configuration is a aluminum-adjuvanted injectable. Possible developments include: • Aqueous formulation, especially for the elderly who may respond well, and/or • Potential for mucosal formulations.
Animal Protection by ID Biomedical Protein Vaccine • Bacteria in lungs decreased up to 10,000-fold in immunized animals on days 2 or 3. • Similar results can be seen with bloodstream infections. • Animals can be protected passively by transfer of immunized human sera. • Basic mechanisms of protection appear to be similar to those induced by current vaccines. Lethal Pneumonia Model Balb/C mice immunized SC x 3, challenged with ~ 103 LD50S. pneumo 14 d later.
Challenges in the Development of a Pneumococcal Group Common Protein Vaccine • Paucity of data regarding the prevalence of protein antibodies and their relation to disease. • Current assays of functional antibodies are optimized for polysaccharide antibodies. • There is no “consensus” regarding protective pneumococcal protein antibody levels. • Clinical efficacy trials for the elderly, will require new thinking about endpoints to be feasible: • Trials targeting IPD will be huge because IPD is rare. • Trials targeting all-cause CAP will be large because of limited efficacy attainable (pneumococci cause only a fraction of CAP). • Trial size and duration are fungible, but any trial must make sense from a corporate perspective.
Issues (1) • CAP with a presumptive etiologic diagnosis represents an endpoint that: • Is of clinical interest and not a rare phenomenon, • Leads to a feasible clinical trials strategy • Requires regulatory assessment of non-cultural diagnostic modalities now licensed for clinical diagnostic use. • Is current validation sufficient? • If not, discussion of validation strategies in the face of a poorly sensitive “gold standard” is needed.
Issues (2) • IDB presumes a placebo-controlled trial cannot be done in the U.S. in the elderly, • 23-PS is little used in many countries with good clinical trials and eldercare infrastructure, so trials can presumptively be done elsewhere, but: • What is the immunogenicity dataset to support U.S. licensure presuming ex-U.S. efficacy? • Would it necessarily require functional assays? Why? • Would it require that the preceding efficacy trial establish a clear-cut protective antibody level to be exceeded? Would equivalent immunogenicity in the U.S. population not suffice?
Issues (3) • How would U.S. licensure for the elderly be approached in the presence of current pneumococcal vaccines? • Would a head-to-head trial of the protein vaccine vs. 23-PS or a conjugate be required? • For IPD, this is in practical terms impossible. • For CAP, the potential comparators have no demonstrated efficacy in RCTs, or consistent effect even in observational studies. • IBD sees no clear requirement for a head-to-head comparison