Download
1 / 19
190 likes | 375 Views
Prison Mental Health Services in South East Queensland as provided by Queensland Health Robert Pedley and friends 17 May 2006. Foucault quoting Esquoril in ‘Madness and Civilisation’ [1965]

E N D
Prison Mental Health Services in South East Queensland as provided by Queensland Health Robert Pedley and friends 17 May 2006
Foucault quoting Esquoril in ‘Madness and Civilisation’ [1965] ‘There are few prisons where the raving mad are not to be found: these unfortunates are chained in the dungeons beside criminals’
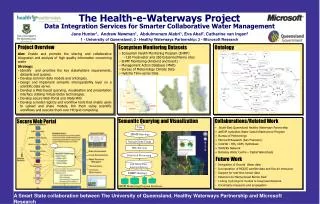
Why? Never a time when the mentally ill were not imprisoned. Our society no different, commensurate rates to comparable societies-with blips If not Q-Health who? Previous systems self contained without links to wider health community-see diagram
QUEENSLAND FORENSIC MENTAL HEALTH SERVICE (QFMHS) MULTIDISCIPLINARY CLINICAL TEAMS 0.9mil 2.3 mil COMMUNITY FORENSIC OUTREACH PROGRAM (CFOS) PRISON MENTAL HEALTH PROGRAM (PMHS) HIGH SECURITY INPATIENT PROGRAM (HSIS) COURT LIAISON SERVICE (CLS)
Who? • Has varied over time but currently we service the 6 secure facilities in SE Queensland. AGCC BWCC Borallon Wolston Woodford Maryborough
Who II ? Numbers are on a steady incline which reflects the overall number of those incarcerated. Generally these numbers reflect the literature on how many seriously mentally ill will be in custody. [With exceptions]
Who III?Dynamic 500-600 • ~ 50 New cases / mth • ~ 50 releases/ mth • 10 new Ax’s – Week • 10 discharges - Week
What [we do and how] We work squarely within the parameters of the expectations placed by legislation and policy on us to treat the mentally ill equally, regardless of where they are to be found Our ambitions are thus broadly commensurate with those of a district mental health service Concentrating on serious Mental Illness rather then broader psychological problems
What [we do and how] II • We triage between 2000-3000 people per year • Accept referrals from absolutely anywhere and from anybody [concentrating on nursing / psychological] • Extremely close links and communication with Court Liaison Service
What [we do and how] III • Palmer inquiry reminds us not to tolerate mental illness in custody. It is contrary to UN standards • Since 1st March 2002 we can access any appropriate AMHS. • Done over 300 times. With relatively few problems. • Taken advantage of 2 or 3 / week • Increasing acceptance of the necessity of this process from AMHS
What [we do and how] IV Treatment in correctional facilities is almost never given involuntarily [there are rare considered exceptions] Initial attempts to introduce multi-disciplinary treatment Attempt to link up with services upon discharge
What Now? Obvious problems in treating serious illness in this environment Comments in various inquiries remarking upon shortcomings New model of funding with increase as of July 2006
What Now II ? Areas of most pressing need include inability to track movements of so many patients with so many movement variables Gains made often entirely undone when people leave custody due to lack of resources or our inability to adequately link people in to services
What Now III ? Investigate how resources would stand expansion of service to farms Enhanced triage and education arm of service Continue collection of data by which to map trends for enhancement of service delivery Transitional case management for the most needy
What Now IV?New funding PMHS 06-07 • State wide clinical director • Building-Infrastructure • Admin support • Vehicles [and access to such] • Case Managers (SE Qld and Northern) • Increased medical coverage • Specific funding for NGO support workers
What Now V?Transitional Case Management • Focus on re-establishing social supports, housing and employment • Facilitating access to Mental Health follow up and intervention • Drug and alcohol support, legal support and financial and social support systems as and when necessary.
What Now VI ? Transitional Case management II • Designed to assist the most complex patients • Imperative that such a model have built in linkages between ourselves and NGO’s • Assist in funding such a model
What Now VII ? Transitional Case management III • Employ and resource transitional case managers • Employ and resource NGO community [mental health] workers • Start discharge process from point of identification
What Now VIII?Transitional Case Management IV Who? • High Risk Group [Mental Health] • Those with considerable treatment needs • Co-morbidity • Substance misuse • Risk of adverse event • Interaction with multiple organisations (DCS/Courts/Legal/DMHS/Health etc)