Download
1 / 54
600 likes | 1.02k Views
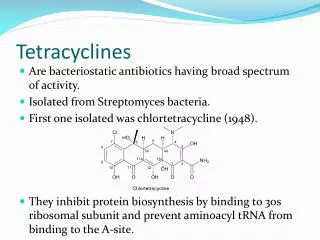
Chapter 42 Tetracyclines and Chloramphenicol. Tetracyclines. Natural: Tetracycline, oxytetracycline, chlortetracycline Semi-synthesized Doxycycline and minocycline. Tetracyclines. Antimicrobial activity Broad-spectrum bacteriostatic antibiotics

E N D
Chapter 42 Tetracyclines and Chloramphenicol
Tetracyclines • Natural: Tetracycline, oxytetracycline, chlortetracycline • Semi-synthesized Doxycycline and minocycline
Tetracyclines • Antimicrobial activity • Broad-spectrum bacteriostatic antibiotics • Many gram-positive and gram-negative bacteria including anaerobes • Rickettsiae, chlamydiae and mycoplasm • Some protozoa: amebas
Tetracyclines • Mechanism of action Tetracyclines bind reversibly to the 30s subunit of bacterial ribosome and block the binding of aminoactyl-tRNA to the acceptor site, prevent the elongation of peptide.
Tetracyclines • Resistance • Production of an efflux pump • Ribosome protection due to production of proteins that interfere with tetracyclines binding to the ribosome • Production of enzyme
Tetracycline • Pharmacokinetics • Absorption: affected by food ,divalent cations(Ca2+, Mg2+ , Fe2+), dairy products and antiacid • Distribution: distribute widely to tissues and body fluids, bind to and damage growing bone and teeth as a result of chelation with calcium • Cross plancental barrier and excrete in milk
Tetracyclines • Clinical uses • Rickettsiae infections : first choice • Chlamydiae pneumoniae • Mycoplasma infection • Relapsing fever: the most effective • Various gram-positive and negative infections • Gastric ulcer and duodenal ulcer caused by Helicobacter pylori in combination regimens
Tetracycline • Adverse reactions • Gastrointestinal adverse effects • Superinfection • Pseudomembranous enterocolitis caused by clostridium difficile • Candida albicans infection • Effects on bony structure and teeth • Teeth: fluorescence, discoloration and enamel dysplasia • Bone: deformity or growth inhibition • Liver and kidney toxicity, photosensitization
Synthesized tetracyclines • Doxycycline and minocycline • Almost completely absorbed • Long-acting: t 1/2 >14h • Higher activity than tetracycline • Effective against tetracycline-resistant bacteria • Low toxicity • Minocycline: the strongest activity/ vestibular disturbance
Antimicrobial activity • Broad-spectrum bacteriostatic antibiotics • Both gram-positive and gram-negative aerobic and anaerobic organisms • Rickettsiae, spirochetes, mycoplasm
Mechanism of action Chloramphenicol is a inhibitor of microbial protein synthesis. It binds reversibly to the 50s subunit of the ribosome and inhibits the peptidyl transferase step of protein synthesis
Pharmacokinetics • Absorption : po • High concentration in CSF • Metabolized in liver
Clinical uses • Bacterial menigitis caused by penicillin-resistant bacteria or penicillin-allergic patients • Typhoid and paratyphoid fever :first choice • Serious rickettsial infections • Topical use for treatment of eye infections
Adverse reactions • Bone marrow disturbances • Reversible suppression of RBC production • Ireversible aplastic anemia • Graybaby syndrome • dose >50mg/kg/d • Gastrointestinal reactions
Synthetic organic antimicrobials • Quinolones • Sulfonamides • Trimethoprim(TMP) • Nitrofurans • Metronidazole
Quinolones • Brief introduction • Antibacterial activity • Mechanism of action • Clinical uses • Adverse reactions
Brief introduction of quinolones • Four generations • First generation:1962 Lesher nalidixic acid • Second generation: 1973 pipemidic acid • Third generation: 1980’s fluoroquinolones • Fourth generation: late 1990’s moxifloxacin(莫西沙星), gatifloxacin(加替沙星)
Nalidixic acid—first generation • Narrow antibacterial spectrum:G- • Poorly absorbed • High adverse reactions
Pipemidic acid--second generation • Higher activity than nalidixic acid • High concentration in urine • Less toxicity than nalidixic acid • Mainly used in gastrointestinal and urinary tract infection
Fluoroquinolones—third generation • Norfloxacin —— 诺氟沙星 • Ciprofloxacin——环丙沙星 • Ofloxacin ——氧氟沙星 • Levoofloxacin——左氧氟沙星 • Lomefloxacin ——洛美沙星 • Fleroxacin ——氟罗沙星 • Sparfloxacin ——司帕沙星
Fluoroquinolones • Antibacterial activity: broad spectrum • Excellent activity against gram-negative aerobic bacteria include enterobacteriaceae, neisseria, pseudomonas, haemophilus(嗜血杆菌属)and campylobacter(弯曲杆菌属)etc • Good activity against gram-positive aerobic bacteria : eg pneumoniae and staphylococci • Mycoplasmas, chlamydiae, mycobaterium tuberculosis, legionella and anaerobes
Quinolones • Mechanism of action • To G-: DNA gyrase A2B2 • To G+: Topo Ⅳ C2E2 • Resistance • Mutation of target : gyrA or parC • Lack of OmpF on membrane • Active efflux pump
Fluoroquinolones • Pharmacokinetics • Absorbed rapidly and completely • Widely distributed • Long T ½ • Low adverse reaction • No cross-resistance with other drugs
Fluoroquinolones • Clinical uses • Urinary and genital tract infections • Respiratory tract infection: Legionella , chlamydia and mycoplasma pneumonia • Bacterial diarrhea caused by shigella, salmonella or campylobacter • Infections of soft-tissues, bones, joint • Tuberculosis : Ofloxacin, Sparfloxacin
Fluoroquinolones • Adverse reactions • Gastrointestinal reaction: nausea, vomiting and diarrhea • CNS: headache, dizziness, insomnia and anxiety, seizure • Allergic effect: skin rash, photosensitivity • Damage growing cartilage and cause arthropathy
Contradications • Pregnancy • Children • CNS disorder • History of epilepsy • Allergic
Nalidixic acid and pipemidic acid • Used only in urinary tract infection • Norfloxacin • The least active in fluoroquinolones, F low • No effects on mycoplasmas, chlamydiae, mycobaterium tuberculosis, legionella • Urinary tract and intestinal tract infections • Ciprofloxacin(悉复欢) • The most active agent in fluoroquinolones against gram-negatives, particularly P. aeruginosa in vitro • No effects on anaerobes
Ofloxacin(泰利必妥) • Improved quality in pharmacokinetics F 89% • Effective on mycobateria, chlamydiae and some anaerobes • Effective on resistant bacteria • Second line agent for tuberculosis • Levo-ofloxacin(可乐必妥,来立信) • F 100% • Superior activity against gram-positive organisms • Effective on mycoplasma, legionella, chlamydia and anaerobes • Lowest toxicity among fluoroquinolones
Lomefloxacin: • F 98% t ½= 7h • To G+ and G-: Similar to ofloxacin • To anaerobes: < ofloxacin • Photosensitivity C8-F • Fleroxacin • F 100%, t ½>10h • Higher activity than ciprofloxacin and ofloxacin (in vivo)
Sparfloxacin • Long-acting t ½>16h • Improved activity against G+ bacteria, anaerobes, mycobateria, mycoplasmas, chlamydiae • Second line agent for tuberculosis • Moxifloxacin fourth generation • F 90% t ½ 12~15h • High activity on most G+ ,G-, anaerobes, mycobateria, mycoplasmas, chlamydiae • Low toxicity
Sulfonamides • Classification • Used in systemic infections • Short-acting: SIZ • Medium-acting: SD, SMZ • Long-acting: SMD • Used in intestinal infections: sulfasalazine • Topic sulfonamides: SD-Ag, SA-Na, SML
Sulfonamides • Antimicrobial activity • Broad-spectrum bacteriostatic agents • Both G+ and G- , chlamydiae trachomatis mycoplasm and some protozoa • Mechanism of action • Inhibit dihydropteroate synthetaseand block bacteria folic acid synthesis
Sulfonamides • Pharmacokinetics • Metabolism: liver • Excretion : kidney pH
Sulfonamides • Adverse effects • Urinary tract disturbance: crystalluria, hematuria, obstruction • Allergic reactions: fever, skin rashes, exfoliative dermatitis, photosensitivity • Hematopoietic disturbances • Granulocytopenia, thrombocytopenia • Hemolytic reactions lack of glucose-6-phosphate dehydrogenase • CNS reaction: headache, vertigo
Sulfonamides • Clinical uses • Urinary tract infection: SIZ, SMZ • Meningococcal meningitis: SD first choice • Ulcerative colitis: sulfasalazine(SASP) • Bacterial dysentery: SMZ • Topical use for trachoma and conjunctivitis: SA-Na • Prevent infections of burn wounds: SD-Ag, SML
Trimethoprim (TMP) • Inhibit bacterial dihydrofolate reductase • Used in combination with sulfonamides: synergism • SMZ+TMP (SMZco,复方新诺明) • Toxicity: teratogenesis
Nitrofurans • Nitrofurantoin • Low blood concentration • Urinary tract infection • Furazolidone • Poorly absorbed • Gastrointestinal tract infection • H.p infection
Metronidazole • Antimicrobial activity and clinical uses • Extraluminal amebiasis: drug of choice • Infections caused by anaerobes • Giardiasis • Trichomoniasis • H.p infection
Metronidazole • Adverse reactions • Gastrointestinal irritation: metallic taste in mouth, nausea, dry mouth • Disulfiram-like effect • CNS: vertigo, parensthesias, ataxia and seizures • Mutagenic and carcinogenic
Tinidazole (替硝唑) • Higher activity 2 • Good pharmacokinetics • Long t 1/2 • Penetrate tissue well • High concentration in CSF 88% • Less toxicity