Download
1 / 50
500 likes | 648 Views
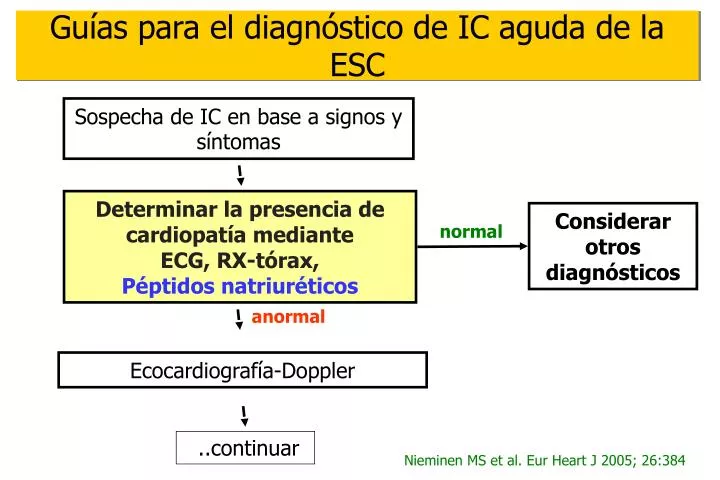
Sospecha de IC en base a signos y síntomas. Considerar otros diagnósticos. normal. anormal. Ecocardiografía-Doppler. ..continuar. Guías para el diagnóstico de IC aguda de la ESC. Determinar la presencia de cardiopatía mediante ECG, RX-tórax, Péptidos natriuréticos.

E N D
Sospecha de IC en base a signos y síntomas Considerar otros diagnósticos normal anormal Ecocardiografía-Doppler ..continuar Guías para el diagnóstico de IC aguda de la ESC Determinar la presencia de cardiopatía mediante ECG, RX-tórax, Péptidos natriuréticos Nieminen MS et al. Eur Heart J 2005; 26:384
ANP BNP Aurícula Localización cardíaca Aurícula y ventrículo Elevada Concentración auricular Baja Secreción cardíaca basal ++ (+) Respuesta de la transcripción genética al estímulo Lenta Rápida Estabilidad mRNA Estable Inestable + +++ Aumento en relación con la insuficiencia cardíaca ANP y BNP: comparación fisiológica
Péptidos natriuréticos: Sintesis -26 amino acid 108 pre-proBNP cardiomiocito 1 108 -26 -1 proBNP signal 1 76 77 108 NT-proBNP sangre BNP
BNP- Diagnosis of acute dyspnea BNP Study: Breathing Not Properly Maisel et al, NEJM 2002;347:161
Estudio ICON • Número total=1256 pacientes • No ICC=536 pacientes • Antecedentes de ICC=55 • No antecedentes de ICC=481 • IC aguda=720 pacientes
ICON Diagnostico y NT-proBNP
ICON 1 0.9 0.8 0.7 Area under the curve=0.94 P<0.00001 Optimal cut: 1160 pg/ml 0.6 Sensitivity (true positives) 0.5 0.4 0.3 0.2 0.1 0 0 0.2 0.4 0.6 0.8 1 1 - Specificity (false positives) Effect of Age on Cut-point Performance • Age <50 years • 84% sensitive/97% specific • Age 50-75 years • 85% sensitive/85% specific • Age >75 years • 94% sensitive/59% specific
1 0.9 0.8 0.7 0.6 Area under the curve=0.99 P<0.00001 Optimal cut: 450 pg/ml 97% sensitive, 93% specific Sensitivity (true positives) 0.5 0.4 0.3 0.2 0.1 0 0 0.2 0.4 0.6 0.8 1 1 - Specificity (false positives) ROC Analysis: Age<50 years
1 0.9 0.8 Area under the curve=0.93 P<0.00001 Optimal cut: 900 pg/ml 89% sensitive, 82% specific 0.7 0.6 0.5 Sensitivity (true positives) 0.4 0.3 0.2 0.1 0 0 0.2 0.4 0.6 0.8 1 1 - Specificity (false positives) ROC Analysis: Age 50-75 years
1 0.9 0.8 0.7 Area under the curve=0.86 P<0.00001 Optimal cut: 1800 pg/ml 85% sensitive, 73% specific 0.6 Sensitivity (true positives) 0.5 0.4 0.3 0.2 0.1 0 0 0.2 0.4 0.6 0.8 1 1 - Specificity (false positives) ROC Analysis: Age >75 years
ICON Predictor OR 95% CI P NT-proBNP elevado* 24.2 12.6-39.3 <0.00001 Edema intersticial en RX 6.7 3.5-12.8 <0.0001 Ausencia de tos 3.7 1.85-7.7 0.0002 Ortopnea 3.5 2.2-5.5 <0.00001 Crepitantes pulmonares 3.0 2.0-4.5 <0.00001 Uso de diuréticos de asa 2.8 1.8-4.4 <0.0001 Antecedentes de ICC 2.8 1.7-4.6 <0.0001 Ausencia de fiebre 2.6 1.7-4.0 <0.0001 Edad 1.6 1.3-1.8 <0.0001 Frecuencia cardiaca 1.01 1.00-1.02 0.004 Análisis de regresión logística MV 22% 36% *NT-proBNP elevado definido como >450 para pacientes <50 años, >900 pg/ml para pacientes 50-75 años, y >1800 pg/ml para pacientes >75 años
Rule Out Cutoff Points International NT-proBNP Collaboration 300 pg/ml, age independent 99% sensitive 60% specific 98% NPV Punto de corte recomendado en las nuevas guías de la ESC
Patient attending the ED with breathlessness History taking, physical exam, ECG, chest X-ray and NTproBNP NTproBNP >450g/mL - patients <50 a >900pg/mL - patients 50-75 a >1800pg/mL - patients >75a NTproBNP <300pg/mL NTproBNP between 2 cut-points Acute CHF likely Acute CHF unlikely Acute CHF less likely Additional tests
The obesity paradox ¿? • Plasma levels of natriuretic peptides appear inversely associated with BMI in both subjects with and without HF. • Natriuretic peptides are lower in overweight and obese patients compared with lean patients Mehra MR et al. JACC 2004;43:1590 Kistorp C et al. Circulation 2005;112:1756. StPeter JV. Clin Chemistry 2006;52:680 Rivera M et al. Eur J Heart Fail 2005;7:1168.
Mechanisms of low NP in obesity Is it a matter of Increased degradation? 22 pts underwent bariatric surgery Parallel increases of BNP and NT-proBNP after weight loss These data refutes the hypothesis that negative correlation between BNP and BMI is due to upregulation of NPR-C because NPR-C do not clear NT-proBNP
Mechanisms of low NP in obesity • Increased degradation • BNP is cleared by NPR-C, abundantly expressed in human adipocytes. • NT-proBNP is not cleared by NPR-C • Reduced synthesis • altered neurohormonal interactions ¿? • Sex steroid hormones ¿? • Substance produced in the lean mass that suppresses either synthesis or release of NP from cardiomyocytes ¿? Das SR et al. Circulation 2005;112:2163 van Kimmenade R et al. JACC 2006;47:886
How obesity affects NT-proBNP in the diagnosis of acute HF?ICON BMI- substudy
Utility of recommended NT-proBNP rule-in and rule-out HF cut-points as a function of BMI
NP and obesity for diagnosing acute HF • Age-adjusted rule-in and age-independent rule-out cut-points for NT-proBNP are equally useful for obese and lean patients Bayes-Genis et al. Arch Intern Med 2006: In press • BMI influences the selection of cut-points for BNP in diagnosing acute HF: • 170 ng/L - lean • 54 ng/L - obese Daniels LB et al. Am Heart J 2006;151:999
How obesity affects the prognostic value of NT-proBNPICON BMI - substudy
Hazard ratios across BMI adjusted for NT-proBNP > 986 ng/L Optimal long-term (1 year) NT-proBNP cut-point: 986ng/L Januzzi JL et al. Arch Intern Med 2006;166:315
K-M survival curves across BMI categories Bayes-Genis et al. Arch Intern Med 2006: In press
BMI, BNP and prognosis Horwich TB et al. JACC 2006;47:85
Diferent prognostic cut-points across BMI Horwich TB et al. JACC 2006;47:85
NP and obesity for long-term risk stratification • One single prognostic cut-point for NT-proBNP (986ng/L) is useful across all BMI categories. Januzzi JL et al. Arch Intern Med 2006;166:315 Bayes-Genis A et al. Arch Intern Med 2006;In press • Optimal BNP cut-points for prediction of death or urgent transplantation are different in the three BMI strata: • 590 ng/L - lean • 491 ng/L - overweight • 343 ng/L - obese Horwich TB et al. JACC 2006;47:85
The obesity paradoxREVISITED In univariable analysis, higher BMI was an independent predictor of survival, with a 4% reduction in the risk of death with every increase of 1 BMI unit (95% CI=0.94-0.99, p=0.002). However, greater BMI was not significantly associated with 1-year mortality once age was added to the model. Thus, the apparent obesity paradox in HF represents an association that is unlikely to be causal
Subestudio Renal de ICON • 720 pacientes con IC aguda • FGR calculado mediante ecuación MDRD • Supervivencia a 60 días • 84 pacientes fallecieron • 606 pacientes vivos Levey et al. Ann Intern Med 1999;130:461-470
Subestudio Renal de ICON • Los pacientes fueron dicotomizados • Según los niveles de NT-proBNP • Concentración mediana = 4647 pg/mL (=548 pmol/L) • Según FGR • > / < 60 ml/min/1.73m² • 51.8% had GFR < 60 ml/min/1.73m²
Predictores independientes de mortalidad en el análisis multivariado
Predictores independientes de mortalidad en el análisis multivariado
Curvas de K-M según FGR y NT-proBNP Van Kimmenade R et al. JACC 2006 In Press
P=0.004 - 15% - 75% - 50% ER 7 d ER 7 d ER 7 d Death of non CV origin Death of CV origin Survivors Percent NTproBNP reduction during admission and prognosis
1,0 - 30% 0,8 Sens: 70% Spec: 84% PPV: 47% NPV 94% Accuracy 82% Sensitivity 0,5 AUC 0.79 (0.69-0.94) p=0.001 0,3 0,0 0,8 0,0 0,3 0,5 1,0 1 - Specificity ROC for NTproBNP reduction during hospitalization
N=182 Decrease 30% - 25% Decrease <30% - ~50% Increase 30% - 80% 6 months Prognosis of NTproBNP reduction during hospitalization for CHF Bettencourt P et al. Circulation 2004;110:2168
A Uneventful Follow-up LVEDD: 69 mm LVEF: 16% Baseline W1 M3 W2 W3 W4 Patient with no events during follow-up
death Hospital admission LVEDD: 73 mm LVEF: 20% Baseline M3 W1 W2 W3 W4 Patient with events during follow-up
What’s next? Resynchronization? i.v. inotropes? Adverse prognosis ??????? Worsening HF Good prognosis outpatient follow-up
