Download
1 / 5
60 likes | 268 Views
2. 1. Start a new, blank presentation with a blank slide layout: File: New Blank presentation Choose an Autolayout: Blank The size of the slide will default to 10” x 7.5” in an “On-screen show” format. Change the format to fit your presentation: File: Page set-up

E N D
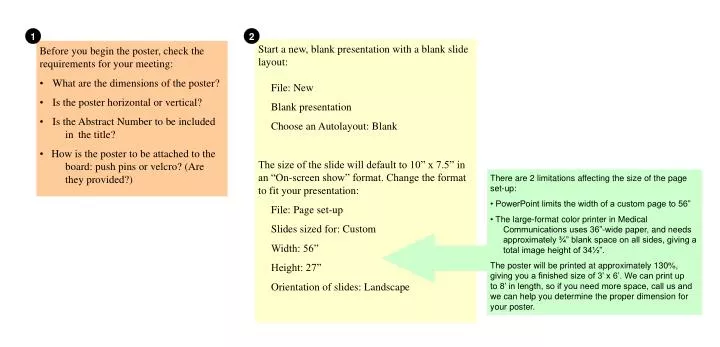
2 1 Start a new, blank presentation with a blank slide layout: File: New Blank presentation Choose an Autolayout: Blank The size of the slide will default to 10” x 7.5” in an “On-screen show” format. Change the format to fit your presentation: File: Page set-up Slides sized for: Custom Width: 56” Height: 27” Orientation of slides: Landscape • Before you begin the poster, check the requirements for your meeting: • What are the dimensions of the poster? • Is the poster horizontal or vertical? • Is the Abstract Number to be included in the title? • How is the poster to be attached to the board: push pins or velcro? (Are they provided?) • There are 2 limitations affecting the size of the page set-up: • PowerPoint limits the width of a custom page to 56” • The large-format color printer in Medical Communications uses 36”-wide paper, and needs approximately ¾” blank space on all sides, giving a total image height of 34½”. • The poster will be printed at approximately 130%, giving you a finished size of 3’ x 6’. We can print up to 8’ in length, so if you need more space, call us and we can help you determine the proper dimension for your poster.
3 If a background color is desired... Format: background Select color from drop-down menu “Fill Effects” offers many options, such as gradients and textures. A word of caution: Don’t allow the background to overpower your text!
14 CASES OF INFANTILE TINEA INFECTION AT A CHILDREN’S HOSPITAL EB Eason and SJ JueDepartment of Pediatrics, Louisiana State University Health Sciences Center, Shreveport, LA. 4 Add a text block (drawn to the approximate size your title will be) and type your title or copy it from the clipboard. The block can be filled with a color or left white. Be sure there’s enough contrast between text color and text block color for the type to be easily read. If you’d like to add a school seal or photograph, it can be added to either side of the title.
14 CASES OF INFANTILE TINEA INFECTION AT A CHILDREN’S HOSPITAL EB Eason and SJ JueDepartment of Pediatrics, Louisiana State University Health Sciences Center, Shreveport, LA. ABSTRACT Purpose of study. Dermatophytic infections have been infrequently reported in young infants. When a case of neonatal tinea capitis was diagnosed at our hospital, a retrospective chart and microbiology record review was performed to determine its prevalence. Methods. Medical records were searched from 1/1/97 - 8/1/99 for infants < 6 months of age with dermatophytic infection. Demographic and clinical information including birth weight, age at presentation, source and identification of isolate, exposure to affected family members with dermatophyte infection or pets, method of treatment, and clinical outcome were obtained. Results. We identified 14 infants (9 males, 5 females) ranging in age from 17-120 days (avg. age 68 days) with tinea capitis due to Trichophyton tonsurans (12) and Microsporum canis (2). (Tables 1,2) Six (43%) of the infants were less than 30 days of age (range 17-25 days). All 12 of the infants with Trichophytontonsurans isolated were black and the 2 infants with Microsporum canis were white. Scalp lesions in 9 infants were described as round and erythematous with scaling and central clearing. One infant had multiple pustular lesions on the scalp and face. None of the patients’ households were reported to have pets. Family members of 3 infants had a history of tinea corporis. Five infants were treated with oral griseofulvin (avg. 24.2 days), 7 with antifungal cream, 8 with antifungal shampoo, and one infant was not treated. Upon follow-up 1 infant initially treated with topical antifungal therapy without resolution was retreated with griseofulvin with unknown outcome, 6 (43%) cases resolved, and 7 (50%) infants were lost to follow-up. (Table 3) Of the 6 infants with resolution of infection, 2 were treated with griseofulvin, 3 received topical antifungal therapy only and 1 infant who was not treated was asymptomatic upon follow-up and may have been treated outside our institution. Conclusion. Tinea capitis in the neonatal period is more common than previously thought and at least in the few neonates described in this report, did not appear to be more extensive or severe than in older children. DISCUSSION The organisms isolated in newborns with tinea capitis have included Microsporum canis (M. canis),Microsporum audouinni, Trichophyton tonsurans, Trichophyton rubrum, Trichophytonmentagrophyte, and Trichophyton violaceum. To our knowledge the youngest newborn with M. canis causing tinea faciei was 6 days old 1 and the first report of T. tonsurans causing tinea capitis and corporis in a newborn was 9 days of age.2 Over a period of 31 months, we identified 14 infants less than 4 months of age with tinea capitis, 6/14 (43%) of whom were neonates ranging in age from 17-25 days. The majority of infants were black and had T. tonsurans isolated from their scalp lesions. The only 2 white infants identified had M. canis isolated from their lesions. Tinea capitis can be transmitted indirectly via fallen hair and desquamated hair cells, as well as by direct contact. T. tonsurans has been isolated from combs, hairbrushes, bedding, and clothing. Asymptomatic carriage has been demonstrated among adults and children living with an index case of tinea capitis and this has led to a growing awareness of asymptomatic carriage as a major reservoir of infection. Of the infants identified in our study, 3 infants had exposure to family members with dermatophyte infection who were likely the initial source of infection. Humans may become infected with M. canis by direct contact with family pets, especially cats and dogs which are the major carriers of this organism. None of the family members had direct contact with family pets. The clinical presentation of these infants was similar to that of older children and consisted primarily of the seborrheic type with circumscribed, erythematous lesions with diffuse scaling, patchy hair loss and a few demonstrated a more inflammatory response with pustular formation. Treatment with oral griseofulvin (10-20 mg/kg/day x 4 weeks) for tinea infection in newborns has been previously reported 3-5 and was tolerated well as it was in the few infants in our study who were treated systemically. The two infants with M. canis infection resolved with topical therapy, one with clotrimazole and one with terbinafine. 5 Add text blocks for each paragraph of text. These should have a white or very light colored background. The headings can make use of a second color. A small black drop shadow can be added to these text blocks, as well. CONCLUSION Tinea capitis in the neonatal period is more common than previously thought and at least in the few neonates described in this report did not appear to be more extensive or severe than in older children. Contact with affected family members or asymptomatic dermatophyte carriers may likely be sources of infection for these infants. INTRODUCTION Tinea capitis is a dermatophytic infection that most commonly occurs in children 3-9 years of age. Trichophyton tonsurans (T. tonsurans) is currently the leading cause of tinea capitis in more than 90% of cases in North and Central America and appears to be more common in black children. Although tinea capitis has been reported previously in young infants, cases in neonates have been rare and primarily consist of isolated case reports.1-8 When a case of tinea capitis was diagnosed in a 17 day old neonate at our hospital, we performed a retrospective chart and microbiology record review in order to determine the incidence of neonatal tinea capitis in our patient population. REFERENCES 1. Jacobs AH, Jacobs PH, Moore N. Tinea faciei due to Microsporum canis in a 6-day-old infant. JAMA 1972;219:1476. 2. Manglini PR, Raman C, Durairaj P, et al. Trichophyton tonsurans infection in a 9-day-old infant. Inter J of Dermatol 1988;27:128. 3. Weston WL, Morelli JG. Neonatal tinea capitis. Pediatr Infect Dis J 1998;17(3):257-258. 4.Ungar SL, Laude TA. Tinea capitis in a newborn caused by two organisms. Pediatr Dermatol 1997;14(3):229-230. 5. Weston WL, Thorne EG. Two cases of tinea in the neonate treated successfully with griseofulvin. Clin Pediatr 1997;16(7):601-602. 6. Ghorpade A, Ramanan C, Durairaj P. Trichophyton mentagrophytes infection in a two-day-old infant. Inter J Dermatol 1991;30:209-210. 7. Gondim-Gonzales HM, Maprunga AC, Melo-Montiero C, Lima AAB. Tinea capitis caused by Microsporum canis in a newborn. Inter J Dermatol 1992;31:368. 8. Alden ER, Chenila SA. Ringworm in an infant. Pediatrics 1969;44 (2):261-262. METHODS Medical records and microbiology records were reviewed from January 1, 1997 thru August 1, 1999 for infants less than six months of age with positive cultures for dermatophytes. Demographic information including the infant’s age, birth weight, gestational age, sex, race, mode of delivery, and environmental factors such as affected family members and household pets were compared. Clinical information studied included the site of the lesion, description of the lesions, organisms isolated by culture, and treatment. The category of treatment was divided into systemic therapy, topical therapy, combined systemic and topical therapy, or no treatment. Outcome was divided into patients with lesions that resolved with therapy, patients who required retreatment, or patients who were lost to follow up. Swabs or scrapings from the scalp lesions of affected children were placed on Dermatophyte Test Media with phenol red indicator and then incubated at 30°C. The media was visually inspected for fungal growth or color change twice a week. Fungi isolated were then identified by colonial and microscopic morphology and stained with lactophenol cotton blue.(figures 1,2) If necessary, the isolate was then subcultured onto Sabouraud’s Dextrose Agar for physiologic testing and further identification.
14 CASES OF INFANTILE TINEA INFECTION AT A CHILDREN’S HOSPITAL EB Eason and SJ JueDepartment of Pediatrics, Louisiana State University Health Sciences Center, Shreveport, LA. 6 Tables, graphs, illustrations and photographs can be placed on white rectangles to match the text blocks. Be sure to include figure legends. Line up text blocks and figures whenever possible, and try to maintain an even spacing between blocks. RESULTS ABSTRACT Purpose of study. Dermatophytic infections have been infrequently reported in young infants. When a case of neonatal tinea capitis was diagnosed at our hospital, a retrospective chart and microbiology record review was performed to determine its prevalence. Methods. Medical records were searched from 1/1/97 - 8/1/99 for infants < 6 months of age with dermatophytic infection. Demographic and clinical information including birth weight, age at presentation, source and identification of isolate, exposure to affected family members with dermatophyte infection or pets, method of treatment, and clinical outcome were obtained. Results. We identified 14 infants (9 males, 5 females) ranging in age from 17-120 days (avg. age 68 days) with tinea capitis due to Trichophyton tonsurans (12) and Microsporum canis (2). (Tables 1,2) Six (43%) of the infants were less than 30 days of age (range 17-25 days). All 12 of the infants with Trichophytontonsurans isolated were black and the 2 infants with Microsporum canis were white. Scalp lesions in 9 infants were described as round and erythematous with scaling and central clearing. One infant had multiple pustular lesions on the scalp and face. None of the patients’ households were reported to have pets. Family members of 3 infants had a history of tinea corporis. Five infants were treated with oral griseofulvin (avg. 24.2 days), 7 with antifungal cream, 8 with antifungal shampoo, and one infant was not treated. Upon follow-up 1 infant initially treated with topical antifungal therapy without resolution was retreated with griseofulvin with unknown outcome, 6 (43%) cases resolved, and 7 (50%) infants were lost to follow-up. (Table 3) Of the 6 infants with resolution of infection, 2 were treated with griseofulvin, 3 received topical antifungal therapy only and 1 infant who was not treated was asymptomatic upon follow-up and may have been treated outside our institution. Conclusion. Tinea capitis in the neonatal period is more common than previously thought and at least in the few neonates described in this report, did not appear to be more extensive or severe than in older children. DISCUSSION The organisms isolated in newborns with tinea capitis have included Microsporum canis (M. canis),Microsporum audouinni, Trichophyton tonsurans, Trichophyton rubrum, Trichophytonmentagrophyte, and Trichophyton violaceum. To our knowledge the youngest newborn with M. canis causing tinea faciei was 6 days old 1 and the first report of T. tonsurans causing tinea capitis and corporis in a newborn was 9 days of age.2 Over a period of 31 months, we identified 14 infants less than 4 months of age with tinea capitis, 6/14 (43%) of whom were neonates ranging in age from 17-25 days. The majority of infants were black and had T. tonsurans isolated from their scalp lesions. The only 2 white infants identified had M. canis isolated from their lesions. Tinea capitis can be transmitted indirectly via fallen hair and desquamated hair cells, as well as by direct contact. T. tonsurans has been isolated from combs, hairbrushes, bedding, and clothing. Asymptomatic carriage has been demonstrated among adults and children living with an index case of tinea capitis and this has led to a growing awareness of asymptomatic carriage as a major reservoir of infection. Of the infants identified in our study, 3 infants had exposure to family members with dermatophyte infection who were likely the initial source of infection. Humans may become infected with M. canis by direct contact with family pets, especially cats and dogs which are the major carriers of this organism. None of the family members had direct contact with family pets. The clinical presentation of these infants was similar to that of older children and consisted primarily of the seborrheic type with circumscribed, erythematous lesions with diffuse scaling, patchy hair loss and a few demonstrated a more inflammatory response with pustular formation. Treatment with oral griseofulvin (10-20 mg/kg/day x 4 weeks) for tinea infection in newborns has been previously reported 3-5 and was tolerated well as it was in the few infants in our study who were treated systemically. The two infants with M. canis infection resolved with topical therapy, one with clotrimazole and one with terbinafine. Table 1. Demographics of 14 Infants with Tinea capitis Case no. Age (days) Sex Race Preterm/full term B. wt. (grams) Fungal isolate Therapy Outcome 1 89 M B term 3955 T. tonsurans griseofulvin + topical antifungal unknown 2 20 F W term 2870 M. canis topical antifungal resolved 3 17 M W term 2495 M. canis topical antifungal resolved 4 80 M B unknown unknown T. tonsurans None resolved 5 20 F B term 3005 T. tonsurans topical antifungal failure; unknown retreated with griseofulvin 6 120 F B term 2755 T. tonsurans topical antifungal unknown 7 120 F B term 3855 T. tonsurans griseofulvin + topical antifungal unknown 8 120 M B preterm 2595 T. tonsurans griseofulvin resolved 9 17 M B term 2775 T. tonsurans topical antifungal resolved 10 90 F B term 3640 T. tonsurans topical antifungal unknown 11 120 M B term 2920 T. tonsurans griseofulvin + topical antifungal resolved 12 25 M B term 2850 T. tonsurans topical antifungal unknown 13 90 M B preterm 2270 T. tonsurans topical antifungal unknown 14 24 M B preterm 2977 T. tonsurans topical antifungal unknown Figure 1 T. tonsurans (microconidia) CONCLUSION Tinea capitis in the neonatal period is more common than previously thought and at least in the few neonates described in this report did not appear to be more extensive or severe than in older children. Contact with affected family members or asymptomatic dermatophyte carriers may likely be sources of infection for these infants. INTRODUCTION Tinea capitis is a dermatophytic infection that most commonly occurs in children 3-9 years of age. Trichophyton tonsurans (T. tonsurans) is currently the leading cause of tinea capitis in more than 90% of cases in North and Central America and appears to be more common in black children. Although tinea capitis has been reported previously in young infants, cases in neonates have been rare and primarily consist of isolated case reports.1-8 When a case of tinea capitis was diagnosed in a 17 day old neonate at our hospital, we performed a retrospective chart and microbiology record review in order to determine the incidence of neonatal tinea capitis in our patient population. Figure 2 M. canis (macroconidia) Table 3. Treatment and Outcome According to Fungal Isolate Table 2. Characteristics of 14 Infants withTinea capitis at LSUHSC Age (days) 68 (average) 17-120 (range) Birth weight (kilograms) 2.98 (average) 2.2-3.8 (range) Sex males females 9 (64%) 5 (36%) Race blacks whites 12 (86%) 2 (14%) Gestational age* Preterm < 37 wks Term > 37 wks 3 (23%) 10(77%) * Gestational age and birth weight for case 4 are unknown. REFERENCES 1. Jacobs AH, Jacobs PH, Moore N. Tinea faciei due to Microsporum canis in a 6-day-old infant. JAMA 1972;219:1476. 2. Manglini PR, Raman C, Durairaj P, et al. Trichophyton tonsurans infection in a 9-day-old infant. Inter J of Dermatol 1988;27:128. 3. Weston WL, Morelli JG. Neonatal tinea capitis. Pediatr Infect Dis J 1998;17(3):257-258. 4.Ungar SL, Laude TA. Tinea capitis in a newborn caused by two organisms. Pediatr Dermatol 1997;14(3):229-230. 5. Weston WL, Thorne EG. Two cases of tinea in the neonate treated successfully with griseofulvin. Clin Pediatr 1997;16(7):601-602. 6. Ghorpade A, Ramanan C, Durairaj P. Trichophyton mentagrophytes infection in a two-day-old infant. Inter J Dermatol 1991;30:209-210. 7. Gondim-Gonzales HM, Maprunga AC, Melo-Montiero C, Lima AAB. Tinea capitis caused by Microsporum canis in a newborn. Inter J Dermatol 1992;31:368. 8. Alden ER, Chenila SA. Ringworm in an infant. Pediatrics 1969;44 (2):261-262. Griseofulvin (1) Resolved (1) Resolved (1) • Trichophytontonsurans (12) METHODS Medical records and microbiology records were reviewed from January 1, 1997 thru August 1, 1999 for infants less than six months of age with positive cultures for dermatophytes. Demographic information including the infant’s age, birth weight, gestational age, sex, race, mode of delivery, and environmental factors such as affected family members and household pets were compared. Clinical information studied included the site of the lesion, description of the lesions, organisms isolated by culture, and treatment. The category of treatment was divided into systemic therapy, topical therapy, combined systemic and topical therapy, or no treatment. Outcome was divided into patients with lesions that resolved with therapy, patients who required retreatment, or patients who were lost to follow up. Swabs or scrapings from the scalp lesions of affected children were placed on Dermatophyte Test Media with phenol red indicator and then incubated at 30°C. The media was visually inspected for fungal growth or color change twice a week. Fungi isolated were then identified by colonial and microscopic morphology and stained with lactophenol cotton blue.(figures 1,2) If necessary, the isolate was then subcultured onto Sabouraud’s Dextrose Agar for physiologic testing and further identification. Topical antifungal (7) Failure (1) Unknown (5) Infants with Tinea capitis (14) Resolved (1) No treatment (1) Resolved (1) Griseofulvin + Topical antifungal (3) Unknown (2) Microsporumcanis (2) Resolved (2) Topical antifungal (2)