Download

1 / 25
250 likes | 267 Views
Explore controversies surrounding cervical spine immobilisation practices and the golden hour concept in emergency rescue operations. Learn about changing protocols, crush injury management, and the impact on patient outcomes.

E N D
Controversies in rescue Tony Smith, Medical Director, St John
Controversies in rescue • Cervical spine immobilisation • The golden hour • Crush injury • Tourniquets • Questions
Cervical spine immobilisation • A controversial area for sometime • We teach our personnel to clear the cervical spine clinically if: • Patient is awake, alert and cooperative • No neck or upper back pain to palpation, in particular no midline bony tenderness • Normal peripheral motor power and sensation • No significant distracting injuries • These are mechanism and age independent • Many patients are able to be cleared clinically
Cervical spine immobilisation • We teach that the role of firm cervical collar is controversial • May cause more harm than good • We teach not to use tape • We teach not to transport on hard boards, unless very short duration • We take a pragmatic approach to the use of head blocks • We take a pragmatic approach to the uncooperative patient • Goal is to minimise movement
Cervical spine immobilisation • Our previous approach was relatively liberal in terms of not placing a firm cervical collar • But still resulted in a significant number of ‘low risk’ patients receiving a firm cervical collar • More neck pain • More radiation to clear the cervical spine • More agitation • Raised intra-cranial pressure • Impaired breathing • Pressure areas • Possible that a firm cervical collar may cause more harm
Why we decided to change • In 2015 ILCOR changed their advice in the first aid section • “We no longer recommend the routine use of a firm cervical collar” • Firm cervical collars may cause more harm than good • Note: there was no new evidence • Resulted in a number of people changing their approach • For example Queensland Ambulance Service • Many were just looking for a reasonable consensus to make a change • Included ambulance sector in NZ
How we decided to change • Ambulance sector working group produced a draft procedure • Significantly reducing the role of the firm cervical collar • Circulated widely for comment • College of Emergency Medicine • College of Intensive Care Medicine • College of Surgeons • Major Trauma Networks • Spinal Cord Impairment Governance Committee • Spinal Society • Emergency Department staff via unit Managers/Charge Nurses • Large amount of feedback • Overwhelmingly in favour of change • Some feedback that we weren't going far enough
Our experience so far • Early days • Lanyards only went on the vehicles in April/May • Training finishing at the end of July • Clinical practice takes time to change • Always lags behind procedures and guidelines • Will be reviewed at the end of 2018
The golden hour • A concept developed by Adams Cowley in the 1980s • Shock Trauma Center in Baltimore • Concept became a mantra • Patients with major trauma arriving in hospital within sixty minutes have a greater chance of survival
The golden hour • Unfortunately not true… • Multiple databases showed no direct correlation between survival rates and time to arrival in hospital • What they did show • Direct correlation between survival rates and time to arrival in the most appropriate hospital • Key issue • No point in a patient with major trauma going to a hospital that cannot meet their treatment needs
The golden hour • What this means in practice • Take the patient to the right hospital whenever feasible, even if further away than the closest hospital • If going to another hospital minimise the time delay to reaching the right hospital • Policies in place for most • Staging in New Zealand
Crush injury • Severe crush injury is rare • Mortality rates are high • A small group of patients deteriorate rapidly when the weight is released • Sometimes called crush syndrome • Actually release syndrome • Cause is controversial
Crush injury and release syndrome • Amount of injury proportional • Weight of the object, amount of body crushed, duration of crush • Damaged and ischaemic muscle • Release of toxins, including myoglobin and potassium • The weight can act as a tourniquet • Systemic toxin release when weight released
Crush injury and release syndrome • General guide: more than a limb for more than an hour • Release the weight as soon as possible • Time is crucial • Prepare for release syndrome • Apply tourniquet/s if possible • Gain IV access and load with IV fluid • Administer calcium and bicarbonate • Consider administering glucose and insulin • Blood likely to be useful • Coordinated approach and good communication • Should release of the weight be deliberately delayed?
Tourniquets • Have always been controversial • Can be life saving • Will cause limb ischaemia • Can cause nerve damage • Can make bleeding worse • Significant use in WW1 and WW2 • Later years not supported
Tourniquets • Newer designs overcome many disadvantages • Clear evidence during recent wars that they save lives • Most ambulance services have introduced them • Including to first responders
Tourniquets • Newer designs overcome many disadvantages • Clear evidence during recent wars that they save lives • Most ambulance services have introduced them • Including to first responders
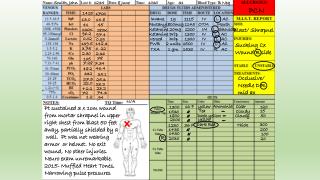
Case example • Van vs truck, trapped • Major injuries to legs that were obviously bleeding • Bilateral tourniquets applied by first responders prior to ambulance arrival • Prolonged extrication
Summary • Cervical spine immobilisation • Changing, role of firm cervical collar is reducing • The golden hour • Doesn't really exist • Important to go to the right hospital • Crush injury • Release syndrome is rare but real • Preparation for and treatment of release syndrome saves lives • Tourniquets • Clearly have a role • Save lives in the hands of first responders