Download
1 / 75
800 likes | 878 Views
Understand the definition, risk factors, and preventive measures of preterm labour, including tocolysis and intrapartum management. Learn about neonatal care and potential complications associated with preterm birth.

E N D
Learning objectives • Definition • Etiology • Risk factors • Diagnosis • Preventive modalities • Plan appropriate treatment modalities • Tocolysis –indication ,C/I , drugs • Principles of intrapartum management • Neonatal care, complications
Definition • PTL is defined as one where labour starts after the gestation of viability (20 -28 wks) and before the 37th completed wks from the first day of LMP (259days).
Preterm is defined as the occurrence of regular uterine contractions (4 or more in 20 minutes or eight or more in one hour) and • Cx changes (effacement equal to or more than 80% and dilatation equal or greater than 2cm) in women with intact fetal membranes and gestational age <37 weeks.
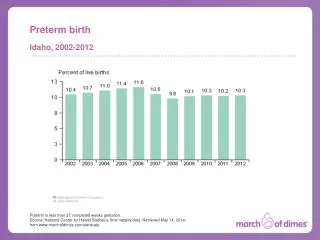
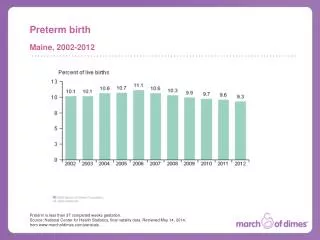
Incidence : 10-15% PTL – significant cause of PN morbidity & motality • Very early <32 wks • Early preterm labour 32-34 wks • Late preterm labour 34-37 wks
Etiology - Maternal factors • Extremes of age • Under nutrition • Poor maternal weight gain • Low SE status • Ethnic differences • Smoking • preg. following ART • Physical / psychological stress • Lack of antenatal care
Etiology -Pregnancy complication • Pre-existing maternal illness • Acute systemic infection in mother, • Preeclampsia, PPROM, APH • Genital infections – BV, beta hemolytic strep • Polyhydramnios, MP, IUFD • Fetal malformation • Asymptomatic bacteriuria /recurrent UTI
Etiology - Obstetric history • Previous preterm birth • Previous first / second trimester loss • Previous induced abortion
Etiology -Uterine factors • Cx insufficiency • Bicornuate uterus • H/o diethyl stilbesterol, submucus fibroid • Iatrogenic • idiopathic
Types of PTL : • Spontaneous PTL • Iatrogenic PTL • Preterm premature rupture of membranes • Threatened PTL • Advanced PTL
Prediction of PTL • Prior preterm birth – three fold increase • Screening for bacterial vaginosis • Ultra sound cx assessment : cx length <25mm at 24 wks of gestation • Fetal fibronectin : > 50 ng/ml • Maternal salivary estriol /plasma corticotropin releasing hormone • Ambulatory uterine activity monitoring
Etiopathogenesis of PTL • 80% of Preterm births are spontaneous • 50% Preterm labor • 30% Preterm premature rupture of the membranes • Pathogenic processes • Activation of the maternal or fetal hypothalamic pituitary axis • Infection • Decidual hemorrhage • Pathologic uterine distention
Activation of the HPA Axis • Premature activation • Major maternal physical/psychologic stress • Stress of uteroplacental vasculopathy • Mechanism • Increased Corticotropin-releasing hormone • Fetal ACTH • Estrogens (incr myometrial gap junctions)
Inflammation • Clinical/subclinical chorioamnionitis • Up to 50% of preterm birth < 30 wks GA • Proinflammatory mediators • maternal/fetal inflammatory response • Activated neutrophils/macrophages • TNF alpha, interleukins (6) • Bacteria • Degradation of fetal membranes • Prostaglandin synthesis
Diagnosis • Regular uterine contractions 4/or > in 20mins. • Eight or > in 60min each should last for 40 seconds • Pelvic pain, low backache • Dilatation • effacement
Management • Prevent • Arrest of PTL • Management of advanced PTL • Care of new born
Prevention • Primary -General measures : improve general health, nutrition, infection • Good antenatal care • Early detection of obstetric compl. • Secondary –screening test, prophylactic treatment • Tertiary care –reduce the PN mobidity & mortality
Progesterone : • 17 hydroxy progesterone caproate given weekly injections – 16-36 weeks. Vaginal progesterone Cerclage : • Cervical insufficiency • USG indicated • Rescue cerclage • Screening for BV in women with previous preterm labour
investigations • History / clinical examination • CBC, CRP, HVS • Urine c/s • USG – fetus / Cx. length
Bed rest, hydration Antenatal steroids : • Between 24-34 weeks gestation • Betamethasone12 mg 2 dose 24 hr apart • dexamethasone 6mg 4 doses 12 hr apart • Risk of antenatal steroid.
Tocolysis : • Main use is to gain time for steroids to act, • delay delivery for at least 48 hrs. • for in utero transfer to tertiary centre
C/I to tocolysis • IUFD, • fetal anomaly • chorioamnionitis • Maternal /fetal condition requiring immediate delivery.
Commonly used tocolytics • Betamimetics • Magnesium sulfate • PGSI –Premature closure of DA/oligohydraminos neontal pul. HTN • Nitric oxide donor • Oxytocin antagonists • Calcium channel blockers
Active management Delivery : • Tertiary centre • CS for preterm breech (lower segment vertical/J shaped) • Cx antibiotics – group B streptococcus • Patient in lateral position Avoid ambulation • Ensure adequate fetal oxygenation • CEFM
Avoid narcotics – epidural is preferred • Episiotomy • Outlet forceps • Cord to be clamped at birth • To shift the baby to NICU under neonatologist
Complications of new born -early • Apnea, • birth asphyxia • RDS • feeding problems, • aspiration • Pul hge • IVH • hypoxic ischemic encephalopathy • Hyperbilirubinemia • NEC • Acidisis • electrolyte imbalance • Infection • birth injuries • Haemorrhagic disease of new born
Late complications • Cerebral palsy • seizures • Retinopathy ofprematurity • Anemia, • mental retardation • Bronchpulmonary dysplasia • PDA, • hearing loss • Malabsorption syn • Nephrocalcinosis, • rickcets • Learning disabilities • Sudden infant death syndrome