Download
1 / 35
360 likes | 745 Views
SURGICAL MANAGEMENT OF UNDESCENDED TESTES Dr SAMAD ZARE Shaheed Sadoughi University of Medical Sciences Yazd;Iran. The anatomical classification of undescended testis : Maldescended testes : lying somewhere along the normal line of descent.

E N D
SURGICAL MANAGEMENT OF UNDESCENDED TESTES Dr SAMAD ZARE ShaheedSadoughi University of Medical Sciences Yazd;Iran
The anatomical classification of undescended testis : Maldescended testes: lying somewhere along the normal line of descent. Ectopic testes: lying outside that line.
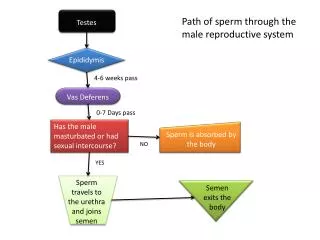
For the full-term boy under the age of 6 mo, proper management includes observation with serial examination because testes may descend spontaneously during early infancy. after the age of 2 yr, histologic deterioration of a UDT (and even its contralateral descended mate) can be observed. It is recommended that surgical orchidolysis and orchidopexyare performed at the latest by 12-18 months of age. To date, it seems that pre- or post-operative hormonal treatment may have a beneficial effect on fertility later in life.
Treatment for undescended testis before puberty decreases the risk of testicular cancer. The relative risk of testicular cancer among those who underwent orchiopexy before reaching 13 years of age was 2.23 And for those treated at 13 years of age or older, the relative risk was 5.40 (15).
Boys with one undescendedtestis have a lower fertility rate but the same paternity rateas boys with bilateral descended testes. Boys with bilateral undescendedtestes have both a lower fertility and paternity rate.
Palpable testis: Surgery for the palpable testis includes orchidofuniculolysis and orchidopexy, via an inguinal approach, with success rates of up to 92% Inguinal orchidopexy: The majority of undescended testes are amenable to a standard inguinal orchidopexyincluding: division of cremastericfibers ligation and division of the processusvaginalis retroperitoneal dissection through the internal ring with division of lateral fascial bands as required.
A proper skin incision for a standard inguinal pediatricorchidopexy: The incision extends from a point corresponding with the position of the internal inguinal ring (midway between the ASIS and the pubic tubercle), medially and transversely within Langer’s lines, to a line vertically through the lateral margin of the scrotum. ASIS, anterior superior iliac spine; PT, pubic tubercle.
An elongated epididymis is commonly found attached to an undescended testis, especially with high inguinal or abdominal testes. It is important to carefully trace the epididymis and vas deferens distally to their most caudal points before dividing the gubernaculum to avoid injuring these structures. Note the extremely long epididymal tail (arrow) extending below the scrotum during this routine inguinal orchidopexy.
With regard to sutures, there should either be no fixation sutures or they should be made between the tunica vaginalis and the dartos musculature. The lymph drainage of a testis that has undergone surgery for orchidopexy has been changed from iliac drainage to iliac and inguinal drainage (important in the event of later malignancy).
Impalpable testis: Some 10–20% of undescended testes are impalpable. In approximately 40% of cases of ‘impalpable testis’ the gonad lies intra-abdominally; in 30% it has ‘vanished’, with vas and vessels ending blindly deep to the internal inguinal ring; in 20% the vas and vessels end blindly within the inguinal canal; ‘nubbin’ and in 10% the testis is normal but concealed within the inguinal canal.
Ultrasound and standard magnetic resonance imaging (MRI) are unreliable for investigating the impalpable testis. Two different groups of investigators have, however, documented the accuracy of gadolinium (Gd)-enhanced MRI, with sedation, fat supressedand DWI MRI and MR Angiography in localizing intra-abdominal testes, canaliculartestes, hypoplastic/atrophic testes, and vanishing testes, with a sensitivity between 96% and 100%
There is a significant chance of finding the testis via an inguinal incision, but in rare cases, it is necessary to search into the abdomen if there are no vessels or vas deferens in the groin. Laparoscopy is the most appropriate way of examining the abdomen for a testis Before starting diagnostic laparoscopy, it is recommended that the child be examined again under general anaesthesia since a previous non-palpable testis might now be palpable under anaesthetic conditions.
An intra-abdominal testis in a 10-year-old boy or older with a normal contralateraltestis should be removed. In bilateral intra-abdominal testes, or in a boy younger than 10 years, a one-stage or two-stage Fowler-Stephens procedure can be performed.
• Testis lying adjacent to the internal inguinal ring – such gonads are usually amenable to a single-stage orchidopexy using a conventional or a preperitoneal approach. An experienced laparoscopist may be able to manipulate the testis towards the inguinal canal so as to assess the feasibility of a single-stage procedure.
Preperitoneal approach (Jones): A skin incision at or slightly higher than for a standard inguinal approach is employed and the oblique abdominal muscles are split to gain access to the peritoneum above the inguinal canal. Thereafter, the testis is mobilisedtransperitoneally and is passed to the scrotum through the inguinal canal or, if necessary, more directly through the posterior wall of the canal medial to the inferior epigastric vessels.
• Testis located on the posterior abdominal wall or ectopically within the pelvis – this calls for a decision as to whether to remove the gonad (either laparoscopically or as an open procedure) or whether to embark upon orchidopexy. Here the options lie between open or laparoscopically assisted orchidopexy, as either a single or a staged procedure.
In the event of a two-stage procedure, the spermatic vessels are either laparoscopically clipped or coagulated proximal to the testis to allow development of the collateral vasculature . The second-stage procedure, in which the testis is brought directly over the symphysis and next to the bladder into the scrotum, can also be performed by laparoscopy 6 months later. The testicular survival rate in a one-stage procedure varies between 50% and 60%, with success rates rising up to 90% in a two-stage procedure.
Microvascularautotransplantationcan also be performed with 90% testicular survival rate. However, the procedure requires a very skilful and experienced surgical technique. Testicular artery and single vein anastomosed to inferior epigastric vessels (or branches).
• Vessels ending blindly together at or above the internal ring – such ‘vanished’ testes presumably result from intrauterine torsion and no further exploration is required. Note that an absent or blind ending vas deferens does not indicate absence of the testis.
• Vas and vessels seen entering the inguinal canal – here it is impossible to be certain whether the canal contains a normal testis or an atrophic nubbin of testicular tissue. Opinion varies on whether inguinal exploration is still mandatory in this situation. Alternatively it has been suggested that inguinal exploration is unnecessary if a nubbin is palpable and the contralateraltestis is hypertrophied (>1.8 cm polar length or 2 ml in volume).
• Failure to visualise blind-ending vessels or testis – in this rare situation, a limited laparotomy is indicated in view of the high risk of subsequent malignancy associated with an undetected intra-abdominal testes left in situ.
Early postoperative • Pain • Bleeding • Hematoma • Local edema • Wound separation • Wound infection. Late postoperative • Testicular malposition or re-ascent • Testicular atrophy • Torsion of testis • Inguinal hernia • Hernia alongside peritonealized vas after Fowler– Stephens orchidopexy – rare complication reported only as isolated case report • Ureteral obstruction due to vasal compression after Fowler–Stephens orchidopexy – rare complication reported only as isolated case report • Impaired spermatogenesis and infertility • Testicular malignancy. COMPLICATIONS:
Retractile Testis The most common form of cryptorchidism and is a normal testis. It has completed the process of descent but tends to pull up out of the scrotum because of the cremastericreflex,whichis particularly strong and universally present in boys between the ages of 2 and 7 yr (3). It can be manipulated into the scrotum, remains in the scrotum (at least temporarily) after its release, and is normal in size. Retractile testes should be monitored during childhood because they can, on some occasions, become truly undescended.
It is not possible to be so confident where the diagnosis lies between ‘high retractile testis’ and true congenital maldescent. In these circumstances the history may be more informative than the examination. Where any doubt exists, regular annual reassessment should be undertaken, and the parents should be advised that the need for surgery cannot be discounted. If, during follow-up, it becomes apparent that a ‘high retractile testis’ is assuming an increasingly abnormal position, hormonal manipulation may be considered as both a diagnostic and a therapeutic trial. In practice, orchidopexy is generally favoured as the primary treatment of choice. In such cases it may be possible to perform this via a scrotal approach.
Ascending testis: The entity of acquired undescended testis, where a previously normal scrotal testis retracts into an ectopic position. There is no consensus on etiology or correct management for these cases; although recent data supports a conservative approach ( until puberty ). Spontaneous descent occurred at puberty in 76% of testes (early puberty in 71.4% of these, 26.5% mid puberty, and 2.1% late puberty) and their expectant policy for the ascending testis has reduced orchidopexy rates in their hospital by 61.8%
Redo orchidopexy: Most papers on repeat orchidopexy include patients who had initial surgery for inguinal hernia, hydrocele, or cryptorchidism and results for these different groups are often amalgamated. A successful result has been documented in 92–100% of cases Re-ascent of the testis requires a redo orchidopexy, which can be performed via the original inguinal incision or with a scrotal approach
Retrograde dissection of the cord structures to gain adequate length. When an inguinal approach is used, a strip of external oblique aponeurosisoverlying the cord may be left attached, thus avoiding difficult dissection between the scarred external oblique. The previously divided hernia sac needs to be separated from the vas and vessels, the peritoneum swept away and retroperitoneal dissection completed. If scar tissue around the deep inguinal ring makes dissection problematic, opening the peritoneum above the ring and dissecting down from above may avoid potential vas or vessel injury. A Prentiss maneuver may be required to achieve a dependent scrotal position and good operative exposure, excellent lighting, optical magnification, and tension-free placement within a scrotal subdartos pouch are important in achieving a satisfactory outcome.
Ectopic Testis The most common site of ectopia is the superficial inguinal pouch of Denis Browne, the space between Scarpa’s fascia and the external oblique fascia above the external inguinal ring. Ectopic descent is thought to result from abnormal development of the gubernaculum or from scrotal inlet obstruction. The accurate diagnosis of an ectopic testis, in contrast to an undescended or retractile testis, is important because the ectopic testis is fixed in position by fibrous attachments. Because it will not descend either spontaneously or with medical therapy, surgery is necessary to place it in the scrotum.
The role of testicular biopsy during routine orchidopexy is controversial. Testicular Biopsy most urologists do not perform testis biopsy during orchidopexy, except in very unusual circumstances. Such circumstances might include orchidopexy in the older child, to exclude a diagnosis of Sertoli cell only (or carcinoma in situ) within the affected testis. The biopsy results may cause unnecessary stress to the patient and family and provide little, if any, useful information for improving future fertility.
POSTOPERATIVE FOLLOW-UP: After orchidopexy, the child should be seen in 2 wk to assess wound healing and check testis position. A second postoperative visit is made 3 mo later to reconfirm testis position and exclude atrophy. Annual scrotal examinations are then recommended during routine visits with the primary care physician. Proper development of secondary sexual characteristics and testicular growth is assessed at puberty, especially for those with a history of bilateral cryptorchidism or delayed surgical correction. Finally, patients are seen after puberty at the age of maturity to teach the technique and the importance of testicular self-examination.
POTENTIAL PITFALLS: 1. Misdiagnosis of a UDT as a retractile testis, which may result in delayed proper management and histologic deterioration. 2. Failure to examine retractile testes annually, which may result in a missed future ascended testis. 3. Iatrogenic tension or torsion on the spermatic cord during orchidopexy, which may lead to orchidopexy failure resulting from testicular retraction or atrophy. 4. Injury to the spermatic cord structures or epididymis during orchidopexy, which may adversely affect testis and tubular function and can easily occur in cases in which there is a long-loop vas deferens or epididymis. 5. Inadequate preservation of collateral blood supply during a FSO, which may result in testicular atrophy. 6. Incomplete surgical exploration for a nonpalpable testis, which may leave a testis in the abdominal cavity or lead to the removal of an inaccurately identified vanished testis from the groin or scrotum.