Download
1 / 14
140 likes | 177 Views
This overview summarizes three clinical studies on the use of sterile vs. non-sterile gloves in managing simple lacerations. The studies by Worral, Bodiwala and George, and Perelman et al. assessed infection rates, antibiotic use, and other outcomes in patients with lacerations repaired using different glove techniques.

E N D
The Use of Sterile Vs. Non-Sterile Gloves in Managing Simple Lacerations Carolyn Phillips MD April 13, 2004
Clinical Studies • Worral, GJ. Repairing skin lacerations: Does sterile technique matter? Can. Fam. Physician. 1987;33:1185-1187. • Bodiwala GG, George TK. Surgical gloves during wound repair in the accident-and-emergency department. Lancet. 1982;2: 91-92. • Perelman et al. Sterile versus nonsterile gloves for repair of uncomplicated lacerations in the Emergency Department: a randomized controlled trial. Ann Emerg Med. 2004;43: 362-370.
Worral • randomized, not controlled, prospective trial performed by Dr. Worral from his rural practice in Canada. • Non-blinded to physician, who both did the suturing and carried out the follow up in the study. • Inclusion criteria: all lacerations were included through the study period.
Worral • 50 patients enrolled, 43 completed study (7 did not complete follow up) • 22 had wounds sutured with full sterile technique including gloves, mask, sterile irrigation and 21 with ‘surgically clean’ technique which was defined as washed hands and arms, tap water irrigation, no mask, no gloves. • Follow up was in Dr. Worral’s office, which adds obvious bias as he was not blinded but at least adds consistent reporting of infection.
Worral • Evaluation: • At follow up, recorded information included infection, antibiotic use, pain or slow healing and need for extra visits or dressings. • Patients were examined at 2 to 3 days after wound repair and then again at suture removal.
Results: Worral • Sterile technique was more likely to cause infection than surgically clean technique (no gloves) in this small study. (10 patients with infection vs. 3). • Five patients of the total 13 infected received antibiotics (4 sterile, 1 surgical). Difference in need for antibiotics or extra visits was not statistically significant.
Bodiwala and George • randomized, prospective trial out of the Leicester Royal Infirmary • Non-blinded to suturer, follow-up wound check blinded to use of gloves • Inclusion criteria: all lacerations were included
Bodiwala and George • 418 patients enrolled, 408 completed study (10 lost due to incomplete data on forms) • 207 had wounds sutured with sterile gloves and 210 with no gloves at all • Follow up was in ED (384 patients) by two senior physicians or via mail-in form from primary physician (34 patients). In one case whether gloves were used or not was not recorded and in nine cases the result in terms of infection was not recorded.
Bodiwala and George • Evaluation: • At follow up, recorded information included interval between suturing and removal of sutures, any use of drugs, underlying disease, and type of accident. • If pus and/or wound dehiscence was present, it was classified as severe infection. • If there was redness and/or a little serous drainage, this was considered a mild infection.
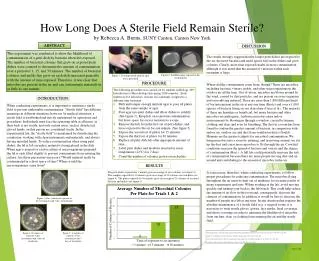
Results: Bodiwala and George • No significant difference between the overall infection rate in the two groups (17.4% in gloves and 17.5 percent in no gloves) or broken down to severe (4.0% vs 4.4%) or mild (13.4% vs 13.1%) infection.
Perelman et al. • A multi-center randomized controlled trial • Blinded to patient and to the follow-up physician, but the suturer knew which type of glove was being used. • Inclusion criteria: older than 1 year of age, any type of uncomplicated soft tissue laceration • Exclusion criteria: presence of diabetes mellitus, renal failure, asplenia, immunodeficiency (congenital, acquired, or receiving immunosuppressive therapy), liver cirrhosis, tendency to form keloid scars, current use of antibiotics or need for prophylactic antibiotics as perceived by the treating physician (eg artificial heart valves, bites, contaminated wounds).
Perelman et al. • 816 patients enrolled, 798 completed study, 18 lost to follow up • 408 received standard intervention (sterile gloves), 408 received experimental intervention (clean-boxed gloves) • Followed up via written data sheet provided to patient at discharge to give to physician providing follow-up care (397 patients) or by phone call (401 patients)
Results: Perelman et al. • Patients were well matched for age, sex, site of wound, injury type and time to repair in hours • There was NO significant difference in wound infection rates between the two groups (6.1% [95% CI 3.8% to 8.4%] in sterile gloves and 4.4% [95% CI 2.4% to 6.4%] in clean-boxed gloves).
HUP ism • The use of sterile gloves does NOT lower infection rates when compared to clean-boxed gloves when repairing simple lacerations