Download
1 / 111
1.14k likes | 2.17k Views
GASTROENTEROLOGY. OBJECTIVES. Upon completion, the student will be able to: Describe the incidence, morbidity and mortality of gastrointestinal emergencies. Identify the risk factors most predisposing to gastrointestinal emergencies.

E N D
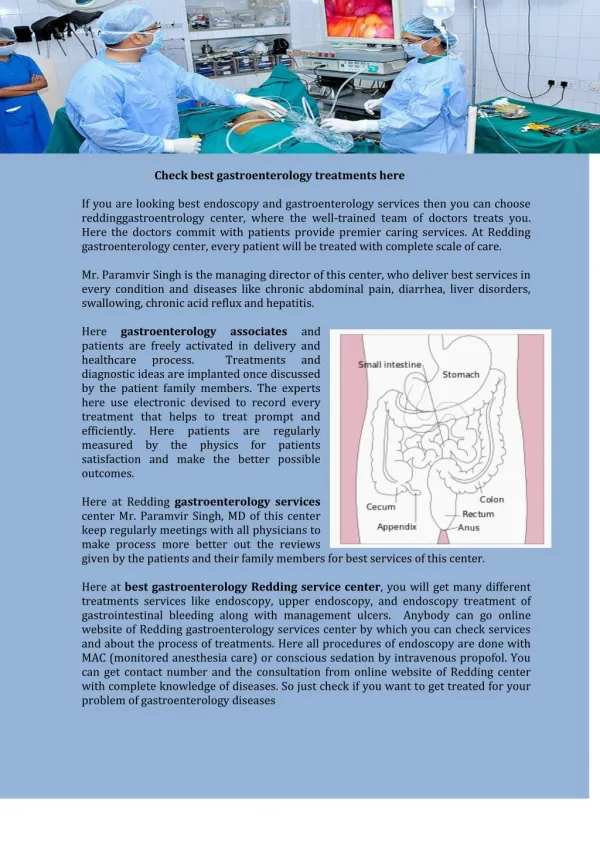
GASTROENTEROLOGY Paramedic Lecture – GI Emergencies
OBJECTIVES • Upon completion, the student will be able to: • Describe the incidence, morbidity and mortality of gastrointestinal emergencies. • Identify the risk factors most predisposing to gastrointestinal emergencies. • Discuss the anatomy and physiology of the gastrointestinal system. • Discuss the pathophysiology of abdominal inflammation and its relationship to acute pain. Paramedic Lecture – GI Emergencies
OBJECTIVES • Define somatic, visceral, and referred pain as they relate to gastroenterology. • Differentiate between hemorrhagic and nonhemorrhagic abdominal pain. • Discuss the signs and symptoms and differentiate between local, general, and peritoneal inflammation relative to acute abdominal pain. • Describe the questioning technique and specific questions when gathering a focused history in patient with abdominal pain. Paramedic Lecture – GI Emergencies
OBJECTIVES • Describe the technique for performing a comprehensive physician examination on a patient complaining of abdominal pain. • Discuss the pathophysiology, assessment findings, and management of the following gastroenterological problems: a) Upper gastrointestinal bleeding b) Lower gastrointestinal bleeding c) Acute gastroenteritis d) Colitis Paramedic Lecture – GI Emergencies
OBJECTIVES e) Gastroenteritis f) Diverticulitis g) Appendicitis h) Ulcer disease i) Bowel obstruction j) Crohn’s disease k) Pancreatitis l) Esophageal varices Paramedic Lecture – GI Emergencies
OBJECTIVES m) Hemorrhoids n) Cholecystitis o) Acute hepatitis • Differentiate between gastrointestinal emergencies based on assessment findings. • Given several scenarios involving patients with abdominal pain and symptoms, provide the appropriate assessment, treatment, and transport. Paramedic Lecture – GI Emergencies
Introduction • Account for 500,000 emergency visits yearly • 300,000 are due to GI bleeds • Will increase because of an aging population • Usually result from an underlying pathologic process that is predictable by risk factors: • Excessive alcohol consumption • Excessive smoking • Increased stress • Ingestion of caustic substances • Poor bowel habits Paramedic Lecture – GI Emergencies
General Pathophysiology • Pain is the hallmark of the acute abdominal emergency. • Three main classifications of abdominal pain: • Visceral • Somatic • Referred Paramedic Lecture – GI Emergencies
Visceral Pain • Originates in the walls of hollow organs, • In the capsules of solid organs, • Or in the visceral peritoneum • Three separate mechanisms can produce this pain: • Inflammation • Distention (being stretched out or inflated) • Ischemia (inadequate blood flow) Paramedic Lecture – GI Emergencies
Visceral Pain • All transmit a pain signal from visceral afferent neural fibers back to the spinal column • Pain is usually not localized to any one specific area • Described as very vague or poorly localized, dull or crampy • Body responds through sympathetic stimulation causing N/V, diaphoresis and tachycardia Paramedic Lecture – GI Emergencies
Somatic Pain • Sharp type of pain that travels along definite neural routes (determined by the dermatomes) to the spinal column • This pain is usually associated with perforations or ruptures of hollow organs • Cause can be bacterial (ruptured appendix or gall bladder) or chemical (perforated ulcer or inflamed pancreas-leakage of acidic juices) • Resulting peritonitis can lead to sepsis, and death Paramedic Lecture – GI Emergencies
Referred Pain • Originates in a region other than where it is felt. • Many neural pathways from various organs pass through or over regions where the organ was formed during embryonic development. • Example: inflammation or injury of the diaphragm will have a referred pain in their necks or shoulders. • Example: dissecting abdominal aortic aneurysm produces pain felt between the shoulder blades. Paramedic Lecture – GI Emergencies
General Assessment • Similar to a trauma assessment with an expanded history. • Remember scene safety and BSI • Observe the scene for clues and/or potential evidence of your pt’s problem: meds, alcohol, ashtrays, emesis buckets, etc.. Paramedic Lecture – GI Emergencies
Scene-Size Up and Initial Assessment • Determine if medical or traumatic cause. • If trauma remember C-spine. • ABC’s as always: With most medical patients, you can check responsiveness and airway by asking the patient his name and chief complaint. Paramedic Lecture – GI Emergencies
History and Physical • History: including SAMPLE • Then move on to History of Present Illness Paramedic Lecture – GI Emergencies
History of Present IllnessOPQRST - ASPN • Onset: when did the pain start, was it sudden or gradual? • Provocation/Palliation: makes the pain worse or better? • Quality: dull, sharp, constant? • Region/radiation: pain travel? • Severity: scale 1-10 • Time: when and how long? • Associated Symptoms • Pertinent Negatives Paramedic Lecture – GI Emergencies
Physical Examination • Patient’s general appearance and posture/position • Complete set of vital signs • Visually inspect the abdomen before palpation (distention, discoloration) • Cullen’s Sign: Periumbilical ecchymosis • Grey-Turners Sign: Ecchymosis in the flank • Remove clothing as necessary • Auscultation and percussion are difficult techniques in a noisy environment Paramedic Lecture – GI Emergencies
Physical Examination • Palpation can give you a large amount of information: • Can define the area of pain and identify the associated organs • Palpate the area of discomfort last • Palpation should be done with gentle pressure, feeling for: • Muscle tension or its absence • Masses, pulsation, tenderness Paramedic Lecture – GI Emergencies
General Treatment • Once assessment, focused history and exam have been completed you now will make treatment and transport decisions. • Monitor ABC’s, high-flow O2, IV access, cardiac monitor • Transport in position of comfort • Provide emotional reassurance • The use of analgesics could limit further evaluation • NOTE: Persistent abdominal pain lasting longer than 6 hours is considered a surgical emergency Paramedic Lecture – GI Emergencies
Specific Illnesses • Broken down into two broad categories: • Upper Gastrointestinal Diseases • Lower Gastrointestinal Diseases • Upper GI consists of: mouth, esophagus, stomach, and duodenum • Lower GI consists of: remainder of small intestine and the large intestine Paramedic Lecture – GI Emergencies
Upper GI Bleeding • Bleeding within the GI tract proximal to the ligament of Treitz • This ligament supports the duodenojejunal junction • Accounts for 300,000 hospitalizations yearly • Mortality of 10%, reasons: • Increasing age of population with associated medical problems • Over-the-counter treatments, until problem becomes severe Paramedic Lecture – GI Emergencies
Upper GI Bleeding • Six major identifiable causes of upper GI bleed: • Peptic ulcer disease • Gastritis • Variceal rupture • Mallory-Weiss syndrome (esophageal laceration, usually secondary to vomiting) • Esophagitis • Duodenitis Paramedic Lecture – GI Emergencies
General Presentation • Complain of some type of abdominal discomfort ranging from a vague burning sensation to an upset stomach, gas pain, or tearing pain in the upper quadrants • N/V • If bleeding is in the upper GI, pt. may have Hematemesis (bloody vomitus) Paramedic Lecture – GI Emergencies
General Presentation • Bleeding passes in to the lower GI tract, pt. may have Melena (tarry, foul smelling stool..partially digested blood) • Bleeding can be light or life-threatening • Part of your assessment should include the “tilt test” (orthostatic hypotension: 10-mmHg change in BP or 20-bpm change in HR when pt. goes from supine to standing) Paramedic Lecture – GI Emergencies
General Presentation • If available the “hematocrit” could be normal in early stages but will definitely drop in the latter stages • Other general complaints include: malaise, syncopal & near-syncopal, tachycardia, and indigestion. Paramedic Lecture – GI Emergencies
General Treatment • Maintain airway, oxygenation and circulatory status • Lateral recumbent position or semi-Fowler’s • High-flow O2 • Two large bore IV’s when you suspect GI bleed • Cardiac Monitor Paramedic Lecture – GI Emergencies
Esophageal Varices • Swollen vein in the esophagus • If they rupture mortality is 35% • Cause is usually a rise in portal pressure, due to impeded circulation through the liver. • This will cause a backup of blood into the left gastric vein and into the esophageal veins. • This will cause the veins to dilate outward, under pressure, and as the engorgement continues, cause them to rupture Paramedic Lecture – GI Emergencies
Esophageal Varices • Primary cause is the consumption of alcohol and the ingestion of caustic substances. • Alcohol consumption can result in cirrhosis of the liver. • This will result in fatty deposits and fibrosis in the liver obstructing portal blood flow. • Caustic substances can erode the esophagus from the inside out, causing hemorrhage of a vessel. Paramedic Lecture – GI Emergencies
Esophageal Varices • Patients usually present initially with painless bleeding and signs of hemodynamic instability. • May complain of hematemesis with bright red blood, dysphagia, and a burning or tearing sensation as the varices continue to bleed. • Clotting time increases because the high portal pressure backs up blood into the spleen, destroying platelets. • Classic signs of shock are common. Paramedic Lecture – GI Emergencies
Esophageal Varices • Treatment should focus on aggressive airway management (suction!), intravenous fluid resuscitation, placing pt. in the shock position, and rapidly transporting to the ED. • ED management may include the use of a Sengstaken-Blakemore tube to tamponade the bleed, endoscopic cauterization, or sclerotherapy (injection of a thrombus-forming drug into the vein itself). Paramedic Lecture – GI Emergencies
Acute Gastroenteritis • Inflammation of the stomach and intestines with associated sudden onset of vomiting and/or diarrhea. • Affects 3-5 million people yearly (worldwide). • 20% of all hospitalized patients. • The inflammation causes hemorrhage and erosion of the mucosal and submucosal layers of the GI tract. Paramedic Lecture – GI Emergencies
Acute Gastroenteritis • Also can damage the villi inside the intestine, which absorb water and nutrients. • The water will now move through the bowel at an increased rate. • Dehydration secondary to diarrhea is a common cause of death. • Volume replacement is the major prehospital intervention to minimize hypovolemia. Paramedic Lecture – GI Emergencies
Acute Gastroenteritis • Alcohol and tobacco abusers are at a high risk for gastritis and gastroenteritis • Also nonsteroidal anti-inflammatory drugs such as aspirin can lead to acute gastritis • Alcohol and tobacco have the same effect on the mucosa as aspirin (breakdown the mucosal surfaces of stomach and GI tract) • Other causes include: stress, chemotherapeutic agents and the ingestion of acidic or alkalotic agents Paramedic Lecture – GI Emergencies
Acute Gastroenteritis • Infections such as salmonellosis and staphylococcus can lead to acute gastroenteritis. • Onset is rapid and severe. • Multiple problems arise: • Diarrhea – leading to dehydration. Especially effects pediatric and geriatric patients. • Stool may show melena or hematochezia (bright red blood from erosion of the lining of the lower GI tract) Paramedic Lecture – GI Emergencies
Acute Gastroenteritis • Hematemesis • Fever • N/V • General malaise • Patient may complain of widespread and diffuse abdominal pain that is not specific to any one region. Paramedic Lecture – GI Emergencies
Acute Gastroenteritis • Treatment is mainly supportive and palliative • Position to decrease the risk of aspiration • Oxygenation • Rehydration • Antiemetics: prochlorperazine (compazine) or promethazine (phenergan) • Electrolyte replacement may be necessary at the hospital Paramedic Lecture – GI Emergencies
Chronic Gastroenteritis • Inflammation of GI mucosa marked by long-term mucosal changes or permanent mucosal damage. • Primarily due to microbial infection. • Most prevalent pathogen in the US is Helicobacter pylori bacillus. • Others include: Escherichia coli, Klebsiella pneumoniae, Enterobacter, Campylobacter jejuni, Vibrio cholerae, Shigella, and Salmonella. Paramedic Lecture – GI Emergencies
Chronic Gastroenteritis • Viral pathogens include: Norwalk virus and rotavirus. • Parasitic causes: protozoa Giardia lamblia, Cryptosporidium parvum, and Cyclosporidium cayetenis. • More common in underdeveloped countries. • Transmitted via the fecal-oral route or through infected food or water. Paramedic Lecture – GI Emergencies
Chronic Gastroenteritis • Commonly present with N/V, fever, diarrhea, abdominal pain, cramping, anorexia, lethargy and if severe, shock. • The H. pylori presents with heartburn, abdominal pain, and gastric ulcers. • Treatment: BSI (protect against cross-contamination), monitoring ABCs and transport. • Medical treatment will require identification of the offending organism. Paramedic Lecture – GI Emergencies
Peptic Ulcers • Erosions caused by gastric acid • Can occur anywhere in the GI tract • Location is based on the area of small intestine involved (ex. duodenal ulcer); gastric ulcers-only in the stomach • Occurs 4 times more frequently in males • Duodenal ulcers occur 2-3 times more often than gastric ulcers Paramedic Lecture – GI Emergencies
Peptic Ulcers • Gastric ulcers more common in patients over 50, work in jobs requiring physical activity • Pain usually increases after eating or with a full stomach and they usually have no pain at night • Duodenal ulcers are more common in patients from 25-50 who are executives or leaders under high stress; possible genetic predisposition • Commonly have pain at night or whenever their stomach is empty Paramedic Lecture – GI Emergencies
Peptic Ulcers • Nonsteroidal anti-inflammatory medications, acid-stimulating products, or Helicobacter pylori bacteria are the most common causes • GI mucosal lining is irritated by hydrochloric acid, and pepsin. Adding any of the above agents increases the irritation. • Treatment is focused on antacid treatment and support of any complications (hemorrhage) Paramedic Lecture – GI Emergencies
Peptic Ulcers • Blocked pancreatic duct can also contribute to duodenal ulcers. This duct releases an alkalotic solution in opposition to the high acid contained in chyme. • Another cause is: Zollinger-Ellison Syndrome: Where an acid-secreting tumor provokes the ulcerations; condition causes stomach to secrete excess HCl acid and pepsin. Paramedic Lecture – GI Emergencies
Peptic Ulcers • Findings on exam can vary: • Chronic ulcers can cause a slow bleed with resulting anemia • Visual inspection of the abdomen is only helpful with a significant bleed • Palpation, the pain may be localized or diffuse • Patients usually have relief of pain after eating or coating their GI tract with a liquid such as milk • Acute, severe pain is probably due to a rupture of the ulcer Paramedic Lecture – GI Emergencies
Peptic Ulcers • Depending on location the patient may have hematemesis or may have melena-colored stool • N/V common • Patient will appear ill with signs of hemodynamic instability • Treatment is based on severity • Position of comfort, psychological support • Oxygenation, IV access for fluid resuscitation • Pharmacological administration and rapid transport • Meds include: Zantac and Pepcid (histamine blockers) and antacids, like Carafate Paramedic Lecture – GI Emergencies
Lower GI Diseases • Lower GI tract consists of the jejunum and ileum of the small intestine, and the entire large intestine, rectum and the anus. Paramedic Lecture – GI Emergencies
Lower GI Bleeding • Bleeding in the GI tract distal to the ligament of Treitz. • Most frequently occur in conjunction with chronic disorders and anatomic changes associated with advanced age. • Most common cause is diverticulosis. • Other causes: colon lesions, rectal lesions, and inflammatory bowel disorders such as ulcerative colitis and Crohn’s disease. Paramedic Lecture – GI Emergencies
Lower GI Bleed • Assessment is identical as with upper GI bleeds • Ask patient whether this is a new or old problem • Frequent complaints with lower GI bleeds include cramping pain that may be described as like a muscle cramp or like gas pain, N/V, and changes in stool • Melenic stool usually indicates a slow bleed • Bright red blood, bleed is very large or has occurred in the distal colon Paramedic Lecture – GI Emergencies