Download
1 / 17
170 likes | 300 Views
INTEGRAL-BASED IDENTIFICATION OF A PHYSIOLOGICAL INSULIN AND GLUCOSE MODEL ON EUGLYCAEMIC CLAMP AND IVGTT TRIALS. T Lotz 1 , J G Chase 1 , K A McAuley 2 , J Lin 1 , J Wong 1 , C E Hann 1 and S Andreassen 3 1 Centre for Bioengineering, University of Canterbury, Christchurch, New Zealand

E N D
INTEGRAL-BASED IDENTIFICATION OF A PHYSIOLOGICAL INSULIN AND GLUCOSE MODEL ON EUGLYCAEMIC CLAMP AND IVGTT TRIALS T Lotz1, J G Chase1, K A McAuley2, J Lin1, J Wong1, C E Hann1 and S Andreassen3 1Centre for Bioengineering, University of Canterbury, Christchurch, New Zealand 2Edgar National Centre for Diabetes Research, University of Otago, Dunedin, New Zealand 3Centre for Model-based Medical Decision Support, Aalborg University, Denmark
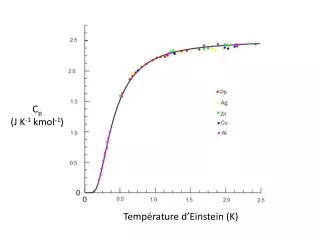
Why model glucose and insulin kinetics? • Glycaemic control from critically ill to diabetic individuals • Tight glycaemic control in ICU reduces mortality by up to 45% • Type 1 and insulin dependent Type 2 diabetes growing rapidly • Diagnosis of insulin resistance • Requires knowledge of glucose and insulin kinetics • Currently, diagnosis occurs ~7 years after initial occurrence • Current models not physiological, difficult to identify, or do not provide high resolution in clinical validation!
ID - Goals • Physiologically accurate model identification • Higher predictive power and resolution • Simple application in a clinical setting • Simple identification without the need of complicated tests (minimal data required) • Use population parameters where possible, fit critical parameters • Computationally efficient
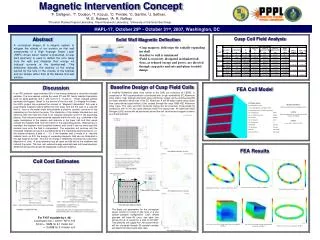
uex PANCREAS nI PLASMA INTERSTITIAL FLUID x·uen CELLS nC diffusion nK nL KIDNEYS LIVER 2-compartment insulin kinetics model + glucose pharmacodynamics GLUCOSE I Q
ID - problems • 2-exponential insulin model but 8 parameters • Physiological solution required Try to identify a priori as many parameters as possible Fit only the most critical parameters! Critical parameters: • Hepatic clearance nL • First pass extraction of endogenous insulin x (if enough resolution in data) • Insulin sensitivity SI • Insulin independent glucose clearance pG • Distribution volumes (if enough resolution in data)
PANCREAS PLASMA VP INTERSTITIAL FLUID VQ uen nI nK KIDNEYS A priori ID - Similarities with C-peptide C-peptide (Van Cauter et al 1992) Equimolar secretion PANCREAS PLASMA VP INTERSTITIAL FLUID VQ x·uen CELLS nC nI Insulin nK nL KIDNEYS LIVER Additional losses
A priori ID – insulin model • Distribution volumes (VP, VQ), transcapillary diffusion (nI), kidney clearance (nK) assumed to match values for C-peptide (similar molecular size, equimolar secretion) • Parameters taken from well validated population model for C-peptide kinetics (Van Cauter et al. 1992) • Saturation of hepatic clearance (αI) fixed from published literature • Clearance by the cells (nC)fixed to achieve ss-concentration gradient between the compartments (Iss/Qss=5/3) (Sjostrand et al 2005) 1 (2) key insulin parameters to be estimated, liver clearance nL(+ first pass hepatic extractionx if data available)
A priori ID – glucose model • Glucose clearance saturation αG= 1/65 (from literature mean, validated in glycemic control trials) • Equilibrium glucose concentration GE= fasting glucose level • Glucose distribution volume VG= 0.19 x body weight (can be estimated if data allows) • Estimate pG, SI, (VG)
Integral-based fitting method • Convex, not starting point dependent • Reduces ID to solving a set of very well known linear equations • 2 steps, first insulin, then glucose • Integrate insulin model between [t0,t1]: • I(t) estimated by interpolating between discrete data • Q(t) known from analytical solution: • Inputs u(t) known (endogenous insulin estimated from C-Peptide)
Integral-based fitting method • Repeat for different time-steps [t0,t1] ... [tn-1,tn]: known known known identify identify solve
Integral-based fitting method • ID glucose model – same approach as shown on insulin solve
Example of result accuracy • Estimation of two parameters in insulin model, nL and x 2D error grid Identified values in 1 iteration! nL= 0.21 x= 0.3 0.3 0.21
Validation on clamps • Euglycaemic clamp trials (N=146) • VG=0.19xbw • uen(t) assumed suppressed • Fitting errors within measurement noise: eG=5.9±6.6% SD; eI=6.2±6.4% SD G(t) I(t) Q(t)
Validation on IVGTT • Data taken from Mari (Diabetologia 1998) • N=5 normal subjects • 22g glucose, 2.2U insulin (5min IV infusion) • Errors in area under curve: eAG=1.6%; eAI=6.7% G(t) I(t) Q(t)
Clinical validation: Dose response test at low and high dosing Same subject on 2 different visits 10g glucose/ 1U insulin 20g glucose/ 2U insulin G(t) G(t) I(t) I(t) Q(t) Q(t)
Conclusions • Physiological insulin kinetics model • Easy a-priori identification with C-peptide population model • Additional fitting of key parameters (1(2) for insulin, 2(3) for glucose) • Integral-based fitting method convex, accurate and not starting point dependent • Great potential for use in clinical applications
Acknowledgements – Questions? Jessica Lin Jason Wong Chris Hann Geoff Shaw Geoff Chase Dominic Lee Kirsten McAuley Jim Mann Steen Andreassen


![>> W1=[1 1 1 1;1 -j -1 j;1 -1 1 -1;1 j -1 -j] W1 =](https://cdn1.slideserve.com/3227081/slide1-dt.jpg)
![C[ i ][j]=A[ i ][1]+B[1][j]](https://cdn2.slideserve.com/3988576/slide1-dt.jpg)