Download
1 / 23
260 likes | 563 Views
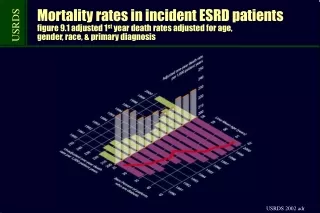
Cardiovascular Disaster in Hemodialysis patients. Pattaraporn MD. Causes of death in prevalent dialysis patients 2008-2010. 41.6%. 26.5%. Cardiovascular Disaster. Sudden death . Unexpected natural death Within a short time period >> 1-24 h Due to cardiac etiology

E N D
Cardiovascular Disaster in Hemodialysis patients Pattaraporn MD.
Causes of death in prevalent dialysis patients 2008-2010 41.6% 26.5%
Sudden death • Unexpected natural death • Within a short time period >> 1-24 h • Due to cardiac etiology • New or more serious symptoms
Possible Mechanisms Responsible for SD in HD Rapid electrolyte shifts/Hypervolemia • Myocardial interstitial fibrosis • Microvessel disease • CHF • CAD/MI • LVH/LV dysfunction QT dispersion Cardiac arrhythmia cardiomyopathy Cardiac arrest Inflammation Ischecmic heart disease Sympathetic overactivity
Left ventricular Hypertrophy and Heart failure Concentric LV hypertrophy Eccentric LV hypertrophy
Left ventricular Hypertrophy and Heart failure • LVH is an powerful indicator of mortality in dialysis patients • Presence of LVH >>> arrhythmia • Left ventricular systolic dysfunction >> arrhythmia Redaelli B: Lancet 1988;ii:305–309.
Myocardial Interstitial fibrosisand Microvessel disease Inadequate capillary density + increased oxygen demand >> relative hypoxia >> fibrosis
Myocardial Interstitial fibrosisand Microvessel disease • Fibrous tissue >> high electrical resistance • Development of atrial and ventricular reentry types of arrhythmias • Risk factor for the development of arrhythmias especially during the dialysis
QT Dispersion • Difference between the longest and shortest QT intervals >> EKG 12 lead • Predict an increased risk of malignant arrhythmias • Normal value of QT dispersion in normal subjects was ≤40 ms • Dialysis patients with QT dispersion > 74 ms >> ventricular arrhythmias or SD • Low K+ and low Ca2+ >> acquired long QT syndrome
Sympathetic overactivity • Heart rate >> myocardial demand supply >> cardiac hypertrophy and fibrosis • Decrease heart rate variability (reflecting autonomic dysfunction) >> increased risk for all-cause and SD in HD
Inflammation • Marker : C-reactive protein, inhibit the hepatic generation of albumin • Reflection of vascular injury VS actually promotes vascular injury ? • High CRP level ( >6 mg/l ) : independent , predictive marker of future myocardial infarction • Herzig, K. A. et al. J. Am. Soc. Nephrol. 12, 814–821 (2001). • Inflammation could trigger SD >> atherosclerosis or direct effect on myocardium
Other factors • Rapid electrolyte shifts • Hypervolemia • Anemia • Dyslipidemia • Hypertension • Calcium/phosphate deposition
Avoiding low K dialysate & rapid electrolyte shifts Prevention of Sudden Death ACEI and ARBs Beta-blocker Implantable defibrillators
Beta-blocker • Reduction of • Cardiac hypertrophy & fibrosis • Antifibrillary activity • Ventricular arrhythmia • Reduced risk of acute MI • Improve Heart rate variability • Increase in baroreflex sensitivity
ACEI andARBs • Reduction of • Cardiac hypertrophy & fibrosis • Fatal arrhythmia
Avoiding low K dialysate & rapidelectrolyte shifts: • To avoid • QT dispersion • Re‐entrant arrhythmias • Premature ventricular extrasystole (VES)
Implantable defibrillators or Implantable CardioverterDefibrillators (ICDs) • Most effective therapy for SCD in the general population • Indication • Survival of cardiac arrest due to VT or VF • Episode of sustained VT causing severe hemodynamic compromise • Episode of sustained VT without hemodynamic compromise + EF 35% • MI + EF 35% + nonsustained VT on 24-h ECG + inducible VT on electrophysiologic testing • MI + EF 30% QRS duration 120 ms on ECG
Implantable defibrillators or Implantable CardioverterDefibrillators (ICDs) • 42% risk reduction for death in dialysis patients with ICDs implanted according to conventional guidelines • Greater risk of device complications • No statistically increase >>> infection or fistula thrombosis • Kidney Int. 2005;68:818-825.