Download
1 / 11
140 likes | 454 Views
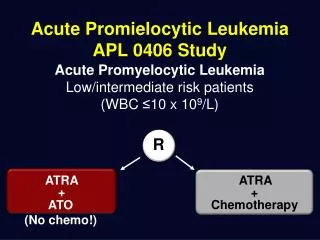
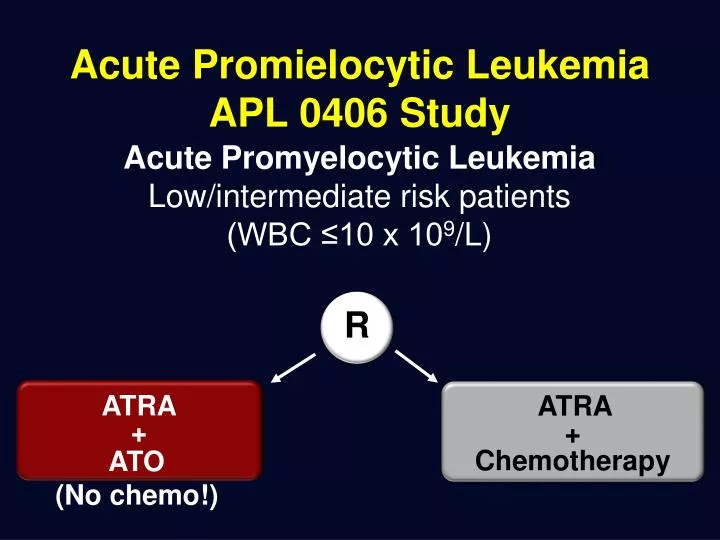
ATRA. +. ATO (No chemo !). Acute Promielocytic Leukemia APL 0406 Study. Acute Promyelocytic Leukemia Low/intermediate risk patients (WBC ≤10 x 10 9 /L). R. ATRA. +. Chemotherapy. 98.7%. 91.1%. Overall survival probability. ATRA+ATO. ATRA+Chemo. Months from diagnosis.

E N D
ATRA + ATO (No chemo!) Acute Promielocytic Leukemia APL 0406 Study Acute Promyelocytic Leukemia Low/intermediate risk patients (WBC ≤10 x 109/L) R ATRA + Chemotherapy
98.7% 91.1% Overall survival probability ATRA+ATO ATRA+Chemo Months from diagnosis Overall Survival p = 0.02
Next Generation Sequencing and identification of genetic defect and possible target for personalized therapy CLL Leukemia TP53 NOTCH1 (PEST) SF3B1 (HEAT) FBXW7 MYD88 XPO1 Multiple Mieloma TP53 B-RAF Hairy Cell Leukemia B-Raf Next Generation Sequencing Acute Myeloid Leukemia MDS EZH2 IDH1 IDH2 TET2 SF1 SF3A1 SF3B1 U2AF1 ASXL1 CBL NPM1 TP53 IDH1/IDH2 EZH2 DNMT3A CEBPA CBL KRAS TET2 RUNX1 BCOR PML-RAR alpha CML or Acute Lymphoblastic Leukemia Myeloprolipherative Disease and Ph- TP53 EZH2 IDH1 IDH2 TET2 CBL KRAS TP53 NOTCH1 FBXW7 IKZF1 BCR-ABL IL7R CRLF2
Imatinib Changed the Therapeutic Landscape for Patients With Ph+ CML Best available therapy5-year OS Imatiniba 93% IFN- or SCT plus 2nd-line imatinibb 71% IFN- or SCTc 63% IFN- 53% Hydroxyurea 46% Busulfan 38% 2010 1.0 0.9 2002-2008, imatiniba 0.8 2000 0.7 1997-2008, IFN- or SCT plus 2nd-line imatinibb 0.6 Survival Probability (All Ph+ CML Disease Phases) 0.5 1990 1995-2008, IFN- or SCTc 0.4 0.3 1986-2003, IFN- 1980 0.2 1983-1994, Hydroxyurea 0.1 1983-1994, Busulfan 0.0 1970 0 2 4 6 8 10 12 14 16 18 20 22 Years After Diagnosis aCML IV; bCML IIIA; cCML III. IFN-, interferon-alpha; OS, overall survival; SCT, stem cell transplant. 1960 Adapted from R. Hehlmann, German CML Study Group.
Landscape of Somatic Mutations in LymphoidNeoplasms Acute Lymphoblastic Leukemia Acute Myeloid Leukemia CLL BCR-ABL like ALL Rossi et al. Blood 2012 Novel rearrangements, copy number alterations, and sequence mutations constitutively activating kinase signaling and dysregulating cytokine receptor signaling. New assessment risk based on genetic alterations New target for new therapy
Genotype-based specific treatment in AML APL [t(15;17)] ATO + ATRA APL0406 GIMEMA/AMLSG/DSIL CBF-AML Dasatinib AMLSG 11-08 FLT3-ITD PKC412 AMLSG 16-10 NPM1mut ATRA +/- GO AMLSG 09-09 Molecular Diagnostics 48h* Azacitidine + intensive induction Allogeneic transplant-strategy Azacitidine maintenance AMLSG 12-09 • All others such as • CN-AML (triple neg) • various • MDS-related AML Clofarabine + ARAC + Idarubicin AMLSG 17-10 Courtesy of Lars Bullinger
Personalized Therapy: a new horizon to get the right target gene(s) for the right therapy, for right patient “at the right dosage” Modified from Modern Pathology (2013) 26, S97–S110, Iacobucci I et al. Curr Cancer Drug Targets. 2013
Association among SNPs and liver toxicity The genotyping profile of 63 patients without liver toxicity (70%) was compared to that of 28 patients (30%) with grade I/II liver toxicity. 10,463 T>C (rs2515641) -333 T>A (rs2070673) 10 11 10q24.3-qter CYP2E1 2 3 4 5 6 7 8 9 1
Suggestions for discussion • As EHA Association we strongly belive that hematological diseases are probably the best suitable model for diffuse patients oriented personalized therapy. • My short presentation of “state of the art” and NGS-PTL project and especially of the new frontiers in blood cancer research strongly suggests that EHA and European haematologists researcher are proud to have increased so much in the last years a “real” applied personalized therapy, to have improved the diagnostic tools for better stratification of leukemic groups, and to have extensively use of target therapy. • Haematology and their research are “fit” with the H2020 and with EAPM aims to improve patients survival with targeted and personalized (individualized) therapy but need for more research funding, more easier access to academic sponsored innovative clinical trials, more regulatory support for conducing “patients oriented” therapy. • We need research funding for blood cancers: it looks like Horizon 2020 gives better opportunities, but these must be translated into call texts.
The personalized “avatar” for each haematological patient to get right target therapy, in a correct dosage, (possible at home) 1 week work CURE “Avatar” Diagnosis: es. BCR-ABL1 like ALL Genome Analyzer II (Illumina/Solexa)/Roche 454 Simulation or Computer assisted decision, in vitro identification of new drugs, etc. Design and apply experimental “individual” and personalized clinical trial (need regulatory EMEA changes ) Extra Rapid (mins not months) Bioinformatics NGS analysis ( e.g. KNOME analysis) done by a medical doctor “Back to bed, soon” reads for each gene RNA/DNA 1 day work Old Classic therapy + ? (ex. Tki, Antibiotic, Vitamin,..) Individual new therapy Old therapy combined with new (eg.TKI) therapy Individual New Target(s) diagnosis relapse
Conclusions The identification of novel diagnostic and prognostic biomarkers, identified through the genomic and transcriptomic signatures, is expected to guide tailored approaches to hema/leukemia and to improve unified deep analysis of He,matological disease complexity as well as the anti-leukemia therapeutic success, guaranteeing the sustainability and efficiency of the healthcare system. unique footprints common path to cure