Download
1 / 18
190 likes | 439 Views
Lymphoedema ....or is it?. Jenny Smith 3 November 2010. Aim. Provide a brief overview of what is meant by lymphoedema and the current recommended management. Learning Outcomes. Define what is meant by the term ‘ lymphoedema ’ Describe characteristic features

E N D
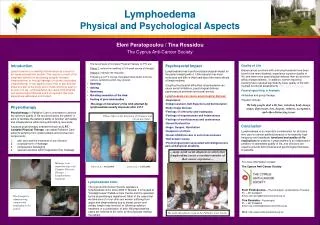
Lymphoedema....or is it? Jenny Smith 3 November 2010
Aim • Provide a brief overview of what is meant by lymphoedema and the current recommended management
Learning Outcomes • Define what is meant by the term ‘lymphoedema’ • Describe characteristic features • List the two main types and the commonest causes • Explain the recommended management
Definitions • What is lymphoedema? • Accumulation of lymphatic fluid in interstitial tissues • Results from abnormal functioning of the lymph system • How is it categorised? • Primary • Secondary
Characteristic Features • Feeling of tightness and heaviness in a limb • Altered sensation, such as pins and needles, shooting pains or feeling of heat • Joint discomfort due to the swelling, e.g. elbow, knee • Tenderness in the groin of an affected leg • Changes in temperature of the limb or affected skin • Reduced range of movement
Making the diagnosis • History • Examination • ? Lymphoscintigraphy • Need to distinguish from lipoedema • Bilateral leg swelling • Nearly always Females • Spares the feet • Not pitting • Can develop lipolymphoedema
Causes • Primary • Underdevelopment • Inherited • Secondary • Trauma • Cancer • Radiotherapy • surgery
Lymphoedema types • Secondary
How common is it? • How common is lymphoedema after surgery for breast cancer (WLE + ANC or mastectomy)? • 14-42% • Why do some develop it after minimal surgery? • Not fully known, ongoing research • ? Pre-disposing factors
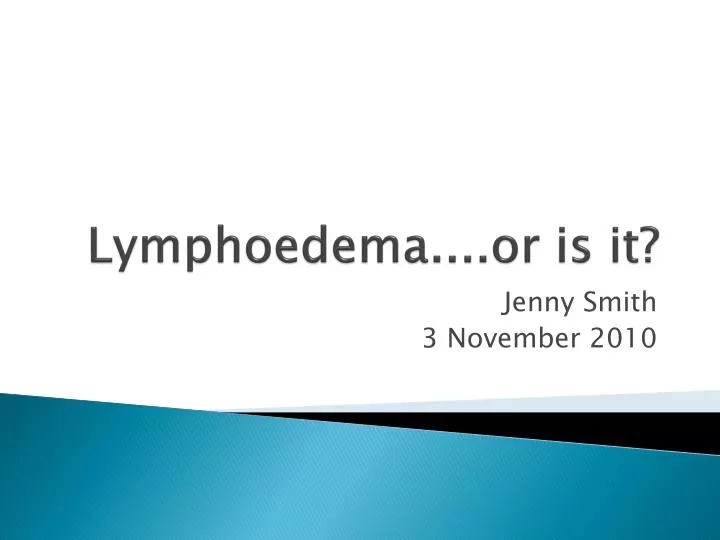
Treatment – mild/moderate • No cure. • Aim reduce the swelling and keep it to a minimum. • Treat in early stages • If a cause is found then the cause needs to be treated, e.g. cancer. • Complex Physical (Lymphatic/Lymphoedema) Therapy (C.P.T./C.L.T.). This regimen consists of 4 main parts. • Skin care – emollients, keratolytics to remove hard, dead skin. • Simple lymphatic drainage – gentle massage, move the swelling out of the affected area. The patient or carer taught technique. • Compression bandaging • Exercise and movement – specially designed programme, maximising lymph drainage without over exertion
Treatment - severe • Manual Lymphatic Drainage – • specialised form massage by trained therapist. Move the skin in specific directions based on the underlying anatomy and physiology of the lymphatic system. • Multi-Layer Lymphoedema Bandaging • Drug therapy • research as to the effectiveness of drug therapy in lymphoedema. Benzopyrenes including flavonoids have been used. Coumarins used. • Surgery – • rare. ?benefit for eyelid or genital swelling. Only surgeons who have experience with lymphoedema and the lymphatic system should perform surgery
Complications • Cellulitis • Prevention • Prompt treatment • British Lymphology Society Consensus Document • http://www.lymphoedema.org/Menu3/consensus_on_cellulitis_aug_10.pdf
Cellulitis • Management of cellulitis in lymphoedema – at home with oral antibiotics • 1. Amoxicillin 500 mg 8 hourly for at least 14 days. • 2. Add Flucloxacillin 500 mg 6 hourly if Staphylococcus aureus infection is suspected e.g. folliculitis, pus formation or crusted dermatitis is present. • 3. If patient is allergic to Penicillin, use Clindamycin 300 mg 6 hourly for at least 14 days
Cellulitis treatment - Hospital • If a patient fails to improve on this regimen or is systemically very unwell, admission to hospital for intravenous antibiotics is recommended. • Prophylactic antibiotics (Penicillin V or Erythromycin) • considered in patients who develop recurrent episodes of cellulitis (=2 per year). Management of the lymphoedema is also reviewed, as a reduction in limb volume is associated with a reduced incidence of cellulitis (Ko et al, 1998).
resources • Leeds Lymphoedema service (Bexley/Wharfedale) • http://www.lymphoedemaleeds.co.uk/ • UK lymph.com • http://www.uklymph.com/ • Cellulitis consensus document: http://www.lymphoedema.org/Menu3/consensus_on_cellulitis_aug_10.pdf • Lymphoedema Framework (2006 a). Best Practice for the Management of lymphoedema. International consensus. London: MEP Ltd • NHS Evidence – supportive and pallitaive care. • http://www.library.nhs.uk/palliative/ViewResource.aspx?resID=271133 • Ko DSC, Lerner R, Klose G et al (1998). Effective treatment of lymphoedema of the extremities. Arch. Surg. 133: 452-458.