Download
1 / 1
10 likes | 172 Views
A Case report: Vaginal Dehiscence during Vaginal delivery in a woman with previous laparoscopic excision of rectovaginal endometriosis Dr. Humera Ansar ( Speciality Trainee ), Leicester Royal Infirmary. UK.

E N D
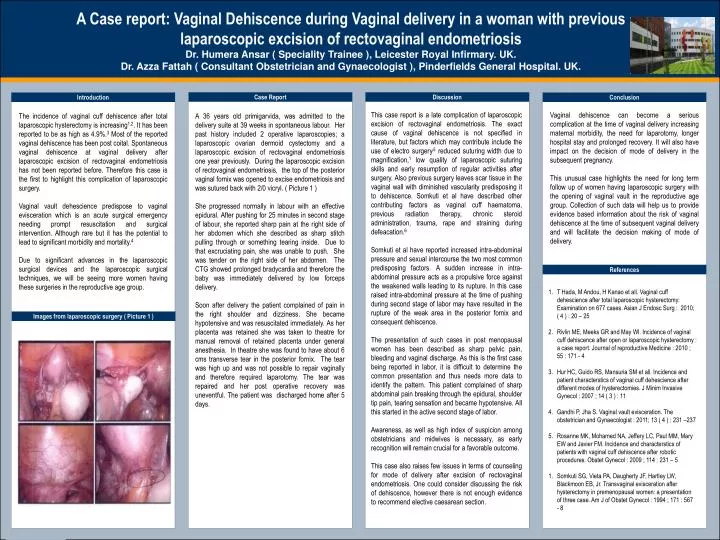
A Case report: Vaginal Dehiscence during Vaginal delivery in a woman with previous laparoscopic excision of rectovaginal endometriosis Dr. Humera Ansar ( Speciality Trainee ), Leicester Royal Infirmary. UK. Dr. Azza Fattah ( Consultant Obstetrician and Gynaecologist ), Pinderfields General Hospital. UK. Case Report Discussion Introduction Conclusion Vaginal dehiscence can become a serious complication at the time of vaginal delivery increasing maternal morbidity, the need for laparotomy, longer hospital stay and prolonged recovery. It will also have impact on the decision of mode of delivery in the subsequent pregnancy. This unusual case highlights the need for long term follow up of women having laparoscopic surgery with the opening of vaginal vault in the reproductive age group. Collection of such data will help us to provide evidence based information about the risk of vaginal dehiscence at the time of subsequent vaginal delivery and will facilitate the decision making of mode of delivery. The incidence of vaginal cuff dehiscence after total laparoscopic hysterectomy is increasing1,2. It has been reported to be as high as 4.9%.3 Most of the reported vaginal dehiscence has been post coital. Spontaneous vaginal dehiscence at vaginal delivery after laparoscopic excision of rectovaginal endometriosis has not been reported before. Therefore this case is the first to highlight this complication of laparoscopic surgery. Vaginal vault dehescience predispose to vaginal evisceration which is an acute surgical emergency needing prompt resuscitation and surgical intervention. Although rare but it has the potential to lead to significant morbidity and mortality.4 Due to significant advances in the laparoscopic surgical devices and the laparoscopic surgical techniques, we will be seeing more women having these surgeries in the reproductive age group. This case report is a late complication of laparoscopic excision of rectovaginal endometriosis. The exact cause of vaginal dehiscence is not specified in literature, but factors which may contribute include the use of electro surgery,5 reduced suturing width due to magnification,1 low quality of laparoscopic suturing skills and early resumption of regular activities after surgery. Also previous surgery leaves scar tissue in the vaginal wall with diminished vascularity predisposing it to dehiscence. Somkuti et al have described other contributing factors as vaginal cuff haematoma, previous radiation therapy, chronic steroid administration, trauma, rape and straining during defeacation.6 Somkuti et al have reported increased intra-abdominal pressure and sexual intercourse the two most common predisposing factors. A sudden increase in intra-abdominal pressure acts as a propulsive force against the weakened walls leading to its rupture. In this case raised intra-abdominal pressure at the time of pushing during second stage of labor may have resulted in the rupture of the weak area in the posterior fornix and consequent dehiscence. The presentation of such cases in post menopausal women has been described as sharp pelvic pain, bleeding and vaginal discharge. As this is the first case being reported in labor, it is difficult to determine the common presentation and thus needs more data to identify the pattern. This patient complained of sharp abdominal pain breaking through the epidural, shoulder tip pain, tearing sensation and became hypotensive. All this started in the active second stage of labor. Awareness, as well as high index of suspicion among obstetricians and midwives is necessary, as early recognition will remain crucial for a favorable outcome. This case also raises few issues in terms of counseling for mode of delivery after excision of rectovaginal endometriosis. One could consider discussing the risk of dehiscence, however there is not enough evidence to recommend elective caesarean section. A 36 years old primigarvida, was admitted to the delivery suite at 39 weeks in spontaneous labour. Her past history included 2 operative laparoscopies; a laparoscopic ovarian dermoid cystectomy and a laparoscopic excision of rectovaginal endometriosis one year previously. During the laparoscopic excision of rectovaginal endometriosis, the top of the posterior vaginal fornix was opened to excise endometriosis and was sutured back with 2/0 vicryl. ( Picture 1 ) She progressed normally in labour with an effective epidural. After pushing for 25 minutes in second stage of labour, she reported sharp pain at the right side of her abdomen which she described as sharp stitch pulling through or something tearing inside. Due to that excruciating pain, she was unable to push. She was tender on the right side of her abdomen. The CTG showed prolonged bradycardia and therefore the baby was immediately delivered by low forceps delivery. Soon after delivery the patient complained of pain in the right shoulder and dizziness. She became hypotensive and was resuscitated immediately. As her placenta was retained she was taken to theatre for manual removal of retained placenta under general anesthesia. In theatre she was found to have about 6 cms transverse tear in the posterior fornix. The tear was high up and was not possible to repair vaginally and therefore required laparotomy. The tear was repaired and her post operative recovery was uneventful. The patient was discharged home after 5 days. References T Hada, M Andou, H Kanao et all. Vaginal cuff dehescience after total laparoscopic hysterectomy: Examination on 677 cases. Asian J Endosc Surg : 2010; ( 4 ) : 20 – 25 Rivlin ME, Meeks GR and May Wl. Incidence of vaginal cuff dehiscence after open or laparoscopic hysterectomy : a case report. Journal of reproductive Medicine : 2010 ; 55 : 171 - 4 Hur HC, Guido RS, Mansuria SM et all. Incidence and patient characterstics of vaginal cuff dehescience after different modes of hysterectomies. J Minim Invasive Gynecol : 2007 ; 14 ( 3 ) : 11 Gandhi P, Jha S. Vaginal vault evisceration. The obstetrician and Gynaecologist : 2011; 13 ( 4 ) : 231 –237 Rosanne MK, Mohamed NA, Jeffery LC, Paul MM, Mary EW and Javier FM. Incidence and characterstics of patients with vaginal cuff dehiscence after robotic procedures. Obstet Gynecol : 2009 ; 114 : 231 – 5 Somkuti SG, Vieta PA, Daugherty JF, Hartley LW, Blackmoon EB, Jr. Transvaginal evisceration after hysterectomy in premenopausal women: a presentation of three case. Am J of Obstet Gynecol : 1994 ; 171 : 567 - 8 Images from laparoscopic surgery ( Picture 1 )






