Download
1 / 4
40 likes | 128 Views
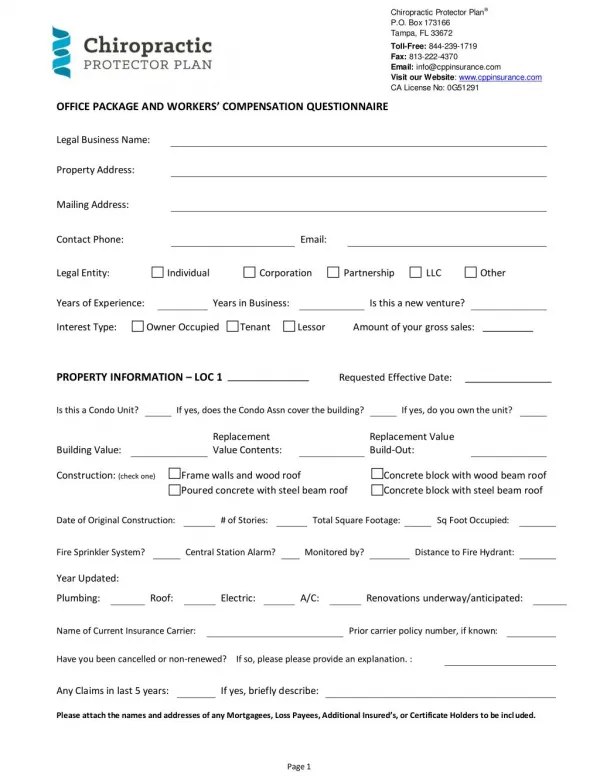
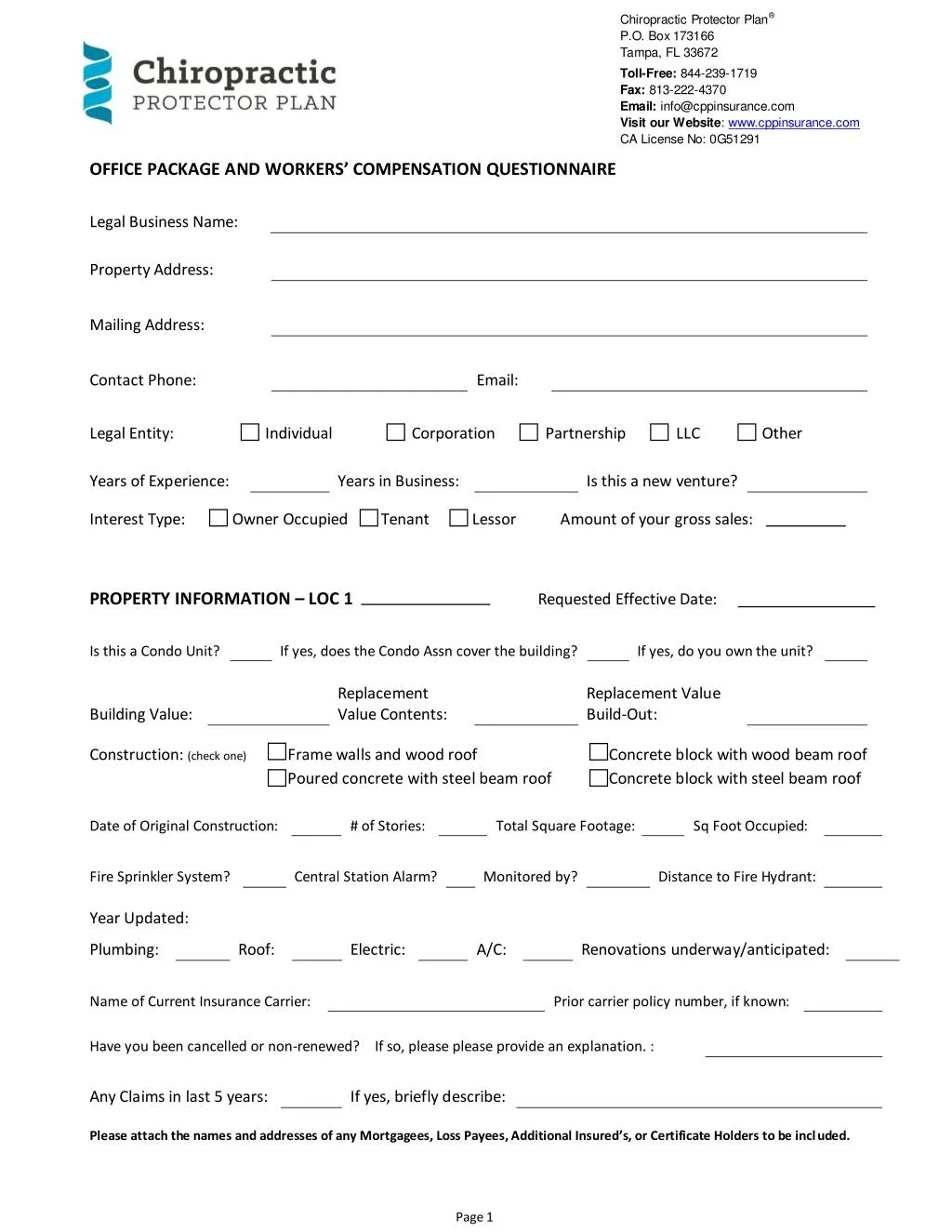
If you are looking for the Chiropractic Insurance the Chiropractic Protector Plan is the best you can get. It offers professional liability, practice insurance and risk management benefits for chiropractic physicians nationwide. Here is the application for Office Package and Workers Compensation Questionnaire.

E N D
Chiropractic Protector Plan® P.O. Box 173166 Tampa, FL 33672 Toll-Free: 844-239-1719 Fax: 813-222-4370 Email: info@cppinsurance.com Visit our Website: www.cppinsurance.com CA License No: 0G51291 OFFICE PACKAGE AND WORKERS’ COMPENSATION QUESTIONNAIRE Legal Business Name: Property Address: Mailing Address: Contact Phone: Email: Legal Entity: Individual Corporation Partnership LLC Other Years of Experience: Interest Type: Owner Occupied Years in Business: Is this a new venture? Tenant Lessor Amount of your gross sales: PROPERTY INFORMATION – LOC 1 Requested Effective Date: Is this a Condo Unit? If yes, does the Condo Assn cover the building? If yes, do you own the unit? Replacement Value Contents: Replacement Value Build-Out: Building Value: Construction: (check one) Frame walls and wood roof Poured concrete with steel beam roof Concrete block with wood beam roof Concrete block with steel beam roof Date of Original Construction: # of Stories: Total Square Footage: Sq Foot Occupied: Fire Sprinkler System? Year Updated: Central Station Alarm? Monitored by? Distance to Fire Hydrant: Plumbing: Roof: Electric: A/C: Renovations underway/anticipated: Name of Current Insurance Carrier: Prior carrier policy number, if known: Have you been cancelled or non-renewed? If so, please please provide an explanation. : Any Claims in last 5 years: If yes, briefly describe: Please attach the names and addresses of any Mortgagees, Loss Payees, Additional Insured’s, or Certificate Holders to be included. Page 1
PROPERTY INFORMATION – LOC 2 Requested Effective Date: Is this a Condo Unit? If yes, does the Condo Assn cover the building? If yes, do you own the unit? Replacement Value Contents: Replacement Value Build-Out: Building Value: Construction: (check one) Frame walls and wood roof Poured concrete with steel beam roof Concrete block with wood beam roof Concrete block with steel beam roof Date of Original Construction: # of Stories: Total Square Footage: Sq Foot Occupied: Fire Sprinkler System? Year Updated: Central Station Alarm? Monitored by? Distance to Fire Hydrant: Plumbing: Roof: Electric: A/C: Renovations underway/anticipated: Name of Current Insurance Carrier: Prior carrier policy number, if known: Have you been cancelled or non-renewed? If so, please please provide an explanation. : Any Claims in last 5 years: PROPERTY INFORMATION – LOC 3 If yes, briefly describe: Requested Effective Date: Is this a Condo Unit? If yes, does the Condo Assn cover the building? If yes, do you own the unit? Replacement Value Contents: Replacement Value Build-Out: Building Value: Construction: (check one) Frame walls and wood roof Poured concrete with steel beam roof Concrete block with wood beam roof Concrete block with steel beam roof Date of Original Construction: # of Stories: Total Square Footage: Sq Foot Occupied: Fire Sprinkler System? Year Updated: Central Station Alarm? Monitored by? Distance to Fire Hydrant: Plumbing: Roof: Electric: A/C: Renovations underway/anticipated: Name of Current Insurance Carrier: Prior carrier policy number, if known: Have you been cancelled or non-renewed? If so, please please provide an explanation. : Any Claims in last 5 years: If yes, briefly describe: Page 2
PROPERTY INFORMATION – LOC 4 Requested Effective Date: Is this a Condo Unit? If yes, does the Condo Assn cover the building? If yes, do you own the unit? Replacement Value Contents: Replacement Value Build-Out: Building Value: Construction: (check one) Frame walls and wood roof Poured concrete with steel beam roof Concrete block with wood beam roof Concrete block with steel beam roof Date of Original Construction: # of Stories: Total Square Footage: Sq Foot Occupied: Fire Sprinkler System? Year Updated: Central Station Alarm? Monitored by? Distance to Fire Hydrant: Plumbing: Roof: Electric: A/C: Renovations underway/anticipated: Name of Current Insurance Carrier: Prior carrier policy number, if known: Have you been cancelled or non-renewed? If so, please please provide an explanation. : Any Claims in last 5 years: PROPERTY INFORMATION – LOC 5 If yes, briefly describe: Requested Effective Date: Is this a Condo Unit? If yes, does the Condo Assn cover the building? If yes, do you own the unit? Replacement Value Contents: Replacement Value Build-Out: Building Value: Construction: (check one) Frame walls and wood roof Poured concrete with steel beam roof Concrete block with wood beam roof Concrete block with steel beam roof Date of Original Construction: # of Stories: Total Square Footage: Sq Foot Occupied: Fire Sprinkler System? Year Updated: Central Station Alarm? Monitored by? Distance to Fire Hydrant: Plumbing: Roof: Electric: A/C: Renovations underway/anticipated: Name of Current Insurance Carrier: Prior carrier policy number, if known: Have you been cancelled or non-renewed? If so, please please provide an explanation. : Any Claims in last 5 years: If yes, briefly describe: Page 3
WORKERS’ COMPENSATION INFORMATION Requested Effective Date: How many total employees do you have? What is your Federal Tax Id #: How many are part-time? What is the gross salary for all employees, excluding Officers: What is the gross salary for Officers? Are Officers/Owners to be included or excluded? List the names of all Officers/Owners: Any claims? If so, please attach a copy of the loss runs. Name of current insurance Carrier: Are health benefits provided? Out of state travel: Do employees dispose of hazardous materials? Salary for those doing grinding of lenses: All other employees: LIMITS: $100,000/$500,000/$100,000 $500,000/$500,000/$500,000 $1,000,000/$1,000,000/$1,000,000 UMBRELLA INFORMATION UMBRELLA LIMITS: $1,000,000 $2,000,000 $3,000,000 Other Notes: