Download

1 / 32
340 likes | 672 Views
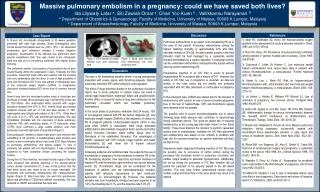
Case report. 報告者:蔡嘉修 時間: 940 922. Present illness. A 45-year-old man had been suffering from diarrhea ,nausea, vomiting, and abdominal discomfort for 1 month before visiting his primary-care physician.

E N D
Case report 報告者:蔡嘉修 時間: 940922
Present illness A 45-year-old man had been suffering from diarrhea ,nausea, vomiting, and abdominal discomfort for 1 month before visiting his primary-care physician. Stool specimens were collected and submitted for routine bacterial culture and examination for ova and parasites. No enteric bacterial pathogens grew in culture seen.
Lab finding A saline wet mount prepared by concentration techniques revealed rare "central-body" parasitic forms which measured 7 to 12 μm. These refractile structures contained large, clear, central areas resembling vacuoles, surrounded by several granules around the periphery.
A permanent smear stained by the trichrome method showed a moderate number of intensely stained blue, vacuolated central-body forms (Fig. 10.1), measuring 8 to 12 μm, with purplish peripheral granules. • In addition, a few amebic trophozoites, measuring 8 to 10 m, with evenly distributed peripheral nuclear chromatin, were seen.
The report from the parasitology laboratory read, "Ova and Parasitology examination revealed Entamoeba hartmanni and moderate Blastocystis hominis."
Question 1 Could either of the parasites listed above be the cause of this patient'sdiarrhea? Explain.
Entamoeba hartmanni Entamoeba hartmanni is a non-pathogenic amoeba with worldwide distribution. Its life cycle is similar to that of E. histolytica but it does not have an invasive stage and does not ingest red blood cells.
Entamoeba hartmanni • Morphology of the trophozoites is similar to those of E. histolytica / dispar but they do not contain ingested red blood cells and the motility is less rapid. • Entamoeba hartmanni is often called a "small histolytica" because these two species share many morphological characteristics, except their size. • The trophozoites of E. hartmanni each have one nucleus with fine peripheral chromatin and a small, often centrally located karyosome. The cytoplasm is finely granular
Entamoeba hartmanni • Trophozoites of E. hartmanni measure usually 8 to 10 µm (range 5 to 12 µm ) and thus are smaller than those of E. histolytica(10 to 60 µm).
Trophozoites of Entamoeba histolytica with ingested erythrocytes (trichrome stain).
Blastocystis homonis Those who do claim to experience symptoms related to blastocystosis claim the following: • Watery diarrhea • Abdominal pain / cramps • Perianal pruritis (itch) • Excessive flatulence
oval cyst-like structures • Blastocystis hominis appear as spherical to oval cyst-like structures • They can vary widely in size (5 to 30 µm; usual range 8 to 10 µm), and typically consist of a central body, or "vacuole" surrounded by a thin rim of cytoplasm containing up to six nuclei.
Blastocystis hominis cyst-like forms stained in trichrome • The sizes vary from 4 µm (A) to 10 µm (F). The vacuoles stain variably from red to blue.
Question 2 What explanation can you give for the difference in quantity of Blastocystis hominis seen in the saline wet mount and in the permanent trichrome stain?
Permanently stained smears are preferred over wet mount preparations because fecal debris may be mistaken for the organisms in the latter.
Question 3 • What accounts for the uncertain taxonomic situation of blastocystis Homonis?
Blastocystis hominis has previously been considered as yeasts, fungi, or ameboid, flagellated, or sporozoan protozoa. Recent molecular studies dealing with the sequence information on the complete SSUrRNA gene, however, have placed B. hominis with an informal group: the stramenopiles (Silberman et al. 1996). Stramenopiles include unicellular and multicellular protistes including brown algae, diatoms, chrysophytes, water molds, slime nets, etc. (Patterson, 1994) Resource:http://www.stanford.edu/class/humbio103/ParaSites2003/Blastocystis%20Hominis/Blastocystis%20Hominis.htm
Question 4 Describe the life cycle of blastocystis hominis.
Life cycle 3 1.The classic form found in human stools is the cyst, which varies tremendously in size from 6 to 40 μm . 2.The thick-walled cyst present in the stools is believed to be responsible for external transmission, possibly by the fecal-oral route through ingestion of contaminated water or food . 3.The cysts infect epithelial cells of the digestive tract and multiply asexually . 4.Vacuolar forms of the parasite give origin to multi vacuolar and ameboid forms.
Life cycle 3 5.The multi-vacuolar develops into a pre-cyst that gives origin to a thin-walled cyst , thought to be responsible for autoinfection. 6.The ameboid form gives origin to a pre-cyst , which develops into thick-walled cyst by schizogony . 7. The thick-walled cyst is excreted in feces . Resource :http://www.dpd.cdc.gov/dpdx/HTML/Blastocystis.asp?body=Frames/A-F/Blastocystis/body_Blastocystis_page1.htm
Question 5 Which treatment might be given for this infection ? How would the treatment differ from that of Entamoeba histolytica?
The treatment of blastocystis hominis • Many believe that this disease is self-limiting and therefore should not be treated. However, upon diagnosis with the disease, patients are usually treated with Metronidazole, which has been effective, but studies have also suggested resistance to this drug • Resource: http://www.stanford.edu/class/humbio103/ParaSites2003/Blastocystis%20Hominis/Blastocystis%20Hominis.htm
The treatment of Entamoeba histolytica • For asymptomatic infections, iodoquinol, paromomycin, or diloxanide furoate (not commercially available in the U.S.) are the drugs of choice. • For symptomatic intestinal disease, or extraintestinal, infections (e.g., hepatic abscess), the drugs of choice are metronidazole or tinidazole, immediately followed by treatment with iodoquinol, paromomycin, or diloxanide furoate.
Question 6 Discuss the epidemiology and prevention of this infection ?
Epidemiology • This disease is not well-tracked, but appears to occur worldwide. • Originally reported as being associated with diarrhea in the tropics and subtropics, more recent reports have show that infections are common in residents of tropical, subtropical, and developing countries. • Immigrants, refugees, and adopted children from developing countries seem to have a higher incidence of infection than adults and children raised from birth in their new community do. • Lower socioeconomic groups or those with lower standards of hygiene have been shown to have higher prevalence rates than the rest of the community. • Young adults appear to have the highest rate of infection.
Prevention The CDC lists the following ways to prevent infection with B. hominis: • Wash hands with soap and water after using the toilet and before handling food. • Avoid water or food that may be contaminated. • Wash and peel all raw vegetables and fruits before eating. • When traveling in countries where the water supply may be unsafe, avoid drinking un-boiled tap water and avoid uncooked foods washed with un-boiled tap water. Bottled or canned carbonated beverages, seltzers, pasteurized fruit drinks, and steaming hot coffee and tea are safe to drink. • If you work in a childcare center where you change diapers, be sure to wash your hands thoroughly with plenty of soap and warm water after every diaper change, even if you wear gloves.















![Case Report # []](https://cdn3.slideserve.com/6989602/slide1-dt.jpg)