Download
1 / 58
670 likes | 1.29k Views
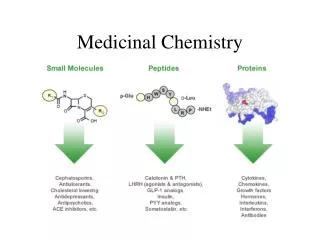
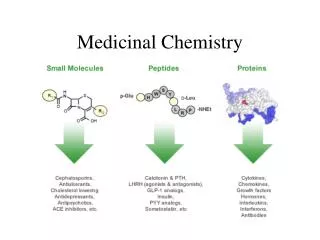
Medicinal Chemistry. Is the science that deals with the design and development of pharmaceutical agents that has a desired biological effect on human body and other living systems. Drug. Is a compound that interact with a biological target to produce a biological response:

E N D
Medicinal Chemistry Is the science that deals with the design and development of pharmaceutical agents that has a desired biological effect on human body and other living systems.
Drug • Is a compound that interact with a biological target to produce a biological response: • Biological target: Human, bacteria, fungi,… • Biological response: desired or undesired. • Sugar, salt, pesticides, herbicides, can be considered as drugs. • Food and fizzy drinks also considered as drugs.
Medicinal chemists concern about the synthesis of new molecules to investigate the relationships between the chemical structure of these compounds and their biological activities.
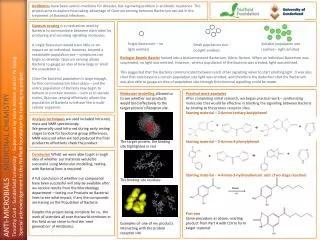
Medicinal chemistry also involves isolation of compounds from natural sources
The Ideal drug must be: • Not toxic. • Effective and potent. • Selective. • Easily administered. • Cheap In Reality, There is no Ideal drug.
Penicillin: one of the safest and most active antibiotics……BUT….. Resistance developed to most of them. • Morphine: a very effective pain killer….. BUT…. May cause tolerance, addiction and respiratory depression. • Heroin: the best pain killer we know….BUT…. addiction developed (still used in terminal cancer).
Drug might be harmful at higher doses: • Therapeutic index: it is the ratio of the dose leads to toxic effect in 50% of cases to that leads to therapeutic effect in 50% of the cases. • Large therapeutic index…… safer drug. • narrow therapeutic index…… more toxic drug.
Poisons can be drugs at lower doses: • Arsenicals: very toxic but used as antiprotozoal agents. • Tubocurarine: used as muscle relaxant.
Selective Toxicity • Selective Drugs: that show toxicity against abnormal cells without affecting normal cells. • Degrees of selectivity: • No effect on normal host cells. • Killing certain microbial strain without affecting others. • Targeting certain metabolic pathway without affecting others.
Drug Targets • they are macromolecules (receptors, enzymes, DNA or transport proteins). • Drugs interact and bind to the binding sites through intermolecular bonds (ionic, H-bonds, Van Der Waals, dipole-dipole and hydrophobic). • The bonds mainly are weak, therefore in most of the cases this binding is reversible.
Human FAS Orlistat
In medicinal chemistry: • Pharmacokinetic: How the drug distribute and reach its target (ADME) and what will happen to the drug • Pharmacodynamic: How the drug interact with its target.
Pharmacokinetics – what the body does to the drug: • How does drug get it into the body? • How long does it take to exert its action? • How long does it stay in the body? • Where does it go to in the body? • Is it metabolised to another form?
Pharmacokinetics Which route? Which formulation? Drug administered Metabolic inactivation Drug absorbed Which barriers to cross? Gut, skin, lungs? Stability at the site of absorption? Pool of non-available Drug in the tissues available Drug in the plasma Excretion • Plasma-protein binding? • Electrostatic charge • Tissue-protein binding? • Fat storage? Passive diffusion? Active transport? Blood-brain barrier penetration? Drug at the site of action
Pharmacokinetic properties • Drug administration: How is the drug to be formulated? If as an injection, is it soluble in aqueous solution? If as a tablet, will it dissolve when released in the gut? • Drug absorption: can the drug pass through the barrier membranes in the GIT? Can it pass through the skin barriers? These barriers are made up in a large part by lipids, so the drug must be sufficiently lipophilic/ unionized to diffuse through them.
Membranes have phospholipids bilayer that act as barriers to the movement of drugs within the body
Pharmacokinetic properties • Drug metabolism: metabolism increases the water solubility of drugs by enzymatically introducing polar functional groups so that they can be excreted: what is the chemistry of the drug? How fast is it inactivated? Is it converted into more active or even toxic components? • Drug excretion: the kidney excretes water-soluble metabolites and the ionized forms of drugs. *
Pharmacodynamics – what the drug does to the body: • What is the therapeutic effect of the drug? • How does it exert its effect? • How does the drug interact with the target? • Can the effect be modified?
More than 90% of drugs have biological targets to bind with in order to exert their pharmacological effects. • Biological targets: are endogenous macromolecules including DNA, RNA, enzymes, receptors, membrane proteins, etc…
DNA Protein
The nature of drug-receptor binding • Either reversible or irreversible. • Reversible binding means that the drug-target complex will dissociate to release the free functioning target. • Irreversible binding means permanently blocking the binding site of the target… irreversible damage.
Interactions involved in drug-receptor interaction • Includes:
Hydrophobic interaction Ionic bonding Dipole-dipole interaction Aromatic interaction Hydrogen bonding
Pharmacokinetics and Pharmacodynamics: are they inter-related?
The answer is definitely yes • If for a reason or another the drug will not reach the target, no pharmacological effect will be observed even if the drug is known to effectively bind to the target active site. • If the drug has a proper pharmacokinetic properties and deposited in enough concentration around the site of action, it must effectively bind to the target to exert its biological effects *
Oral availability • Oral availability or bioavailability measures the fraction of the drug being absorbed into the blood circulation. • Factors affecting oral availability: • Chemical nature of drug (lipophilicity and ionization state). • Water solubility. • Oral stability. • Physiological factors.
Oral stability • Oral stable drugs must be: • Chemically stable toward the GIT conditions; acidic stomach and basic intestine. • Enzymatically stable (first-pass metabolism): stable toward the digestive and metabolizing enzymes such as esterase, amidase and oxidase enzymes. • If the drug is orally unstable it will not be available to be absorbed…..low oral availability.
Oral stability • First pass metabolism does not mean only liver metabolism of orally administered drugs before the drug being deposited in blood. • It covers all metabolic transformation happened to the drug after oral administration before reaching the systemic circulation.
Oral stability • First pass metabolism includes: • All Oral cavity enzymes such as amylase and lingual lipase • Stomach pepsinogen • All GIT proteolytic enzymes. • All Intestinal hydrolase enzymes such as esterase, amidase and carbohydases. • All intestinal lipases and reductase enzymes. *
Orally active agents are drugs either active locally in the GIT lumen (such as in the case of gastroenteritis) or must be absorbed into the blood circulation. • Factors affecting oral activity: • Chemical and enzymatic stability of drugs. • The physiological nature of the GIT lumen. • The same factors affecting the oral availability in the case of systemically active agents. • Orally activity
Systemically active agents must be stable in the GIT as well as during the first pass metabolism if reaching the liver before the blood circulation. • The locally acting agents must be just stable in the GIT, it does not necessarily absorbed through intestinal membrane, they will just act locally: • Given in active form. • Given as prodrug…activated in GIT by special enzymatic reactions • Orally activity
Example: • Paromomycin is one of the aminoglycosides that is widely used in GIT infections caused by salmonella, Shigella and Amoeba. • It is active after oral administration although it has a very limited oral absorption (highly polar compound). • It will only work locally. • Orally activity
Example: • Sulfasalazine; a commonly used drug in ulcerative colitis, although it will be given orally, small quantity will be absorbed. • It will be reduced by colorectal azoreductase to give the active sulfapyridine and P-aminosalicylic acid…both are active • Orally activity
Tissue availability means the amount of the drug that reached the site of action or the target tissue. • In most cases, tissue availability is lower than the oral availability due to one of the following factors: • Extensive drug metabolism. • Blood protein binding. • Rapid drug excretion. • Fat deposition of drug. • Many barriers to penetrate to reach the site of action. • Tissue Availability *
The molecular properties of drugs • It is the physicochemical properties of drugs. • These properties fundamentally affect every thing the drug does to the body (the pharmacodynamic aspects) and what the body does to drugs (the pharmacokinetic aspects). • the molecular properties also determine which dosage form and the route of administration is suitable for the given drug.
Molecular properties of interests • Partition coefficient. • Dissociation constant (degree of ionization). • Solubility (aqueous and fat solubility). • Chemical stability. • Biological stability (metabolic profile of drugs).
Drug solubility • Is drug soluble enough in the GIT content? • Is it soluble enough in blood to be given parenterally? • More water soluble drug in blood….large volume of distribution. • More water soluble drugs…poor penetration into CNS through the lipophilic blood brain barrier.
More water soluble drugs…poor penetration into CNS through the lipophilic blood brain barrier. • As a result, very limited number of drugs can act on CNS.