Download
1 / 53
530 likes | 544 Views
This guide provides detailed instructions on how to properly set up an EKG, including lead placement, lead types, and signal interpretation. Ensure accurate readings and improve diagnostic abilities with this comprehensive resource.

E N D
EKG readings • There must be a full 12 leads labelled and recorded – includes the rhythm strip, usually from lead II. • The baseline must be stable and not wandering. • Leads must be well attached, even if it means shaving a hairy chest. • There should be little interference from skeletal muscle. The patient must be relaxed and comfortable.
EKG Set-up LEFT ARM RIGHT ARM • attach three limb leads – I, II and III (also the basis for the leads aVR, aVL, aVF) • the 3 limb leads form an imaginary inverted triangle over the heart = Einthoven’s triangle -3 LIMB LEADS (I,II,III) -3 AUGMENTED LEADS (aVR, aVL, aVF) -6 CHEST LEADS (V1 – V6) EINTHOVEN’s TRIANGLE LEFT LEG
EKG Set-up • There should be a square wave calibration to show that 1mV is equivalent to 1cm in height. • Speed should be 25mm/sec. Hence 1 large square is 200msec and 1 small square is 40msec.
The Leads • for the EKG – electrodes are paired • output from each pair = lead • lead = tracing of the voltage difference between two electrodes • at rest – heart muscle has a –ve charge • becomes +ve as it depolarizes • the EKG measures the depolarization “wave” as the voltage increases or decreases between two electrodes placed on either side of the heart
The Leads • leads are either unipolar or bipolar • bipolar = have two poles – one is positive, the other is negative • leads I, II & III • unipolar = have two poles – one is positive, the second is the Wilson’s Central terminal (-ve) • aVR, aVF, aVL, V1 – V6 WCT -ve • Wilson’s Central terminal (-ve terminal) = average of the three limb leads • average potential over the entire body
Leads cont… • limb leads = I, II and III • lead I = voltage difference between LA and RA (I = LA-RA) • depolarization wave spreads from right side of heart to left • lead II = voltage difference between LL and RA (II = LL-RA) • spread from right side of heart toward apex • lead III = voltage difference between LL and LA (III = LL-LA) • spread from left side of heart to apex
augmented leads = aVR, aVL, aVF • also called Goldberg’s leads • derived from the 3 limb leads • these leads use the WCT as the –ve electrode • they are positive electrodes that examine the heart from different angles • signal is too small to be useful when the WCT is used as the –ve electrode – so the signal must be amplified or augmented
Augmented Leads: In case you’re curious to know • avR = +ve electrode is on the right arm, -ve electrode is LA + LL – this augments the signal strength of the RA electrode • aVR = (I + II)/2 • aVL = +ve electrode is on the left arm, -ve electrode is RA + LL – this augments the signal strength of the LA electrode • aVL = 1-II/2 • avF = +ve electrode is on the left leg, -ve electrode is LA + RA – this augments the signal strength of the LL electrode • aVF = II-I/2
Precordial or Chest leads • V1 to V6 = chest leads • because of close proximity to the heart – do not require augmentation • use the WCT as the –ve electrode • unipolar leads
Axis • overall direction of the depolarization wave is called the axis • Axis = general direction of the heart’s depolarization wavefront • related to where the bulk of the heart’s muscle is – generally the left ventricle • oriented from the right shoulder to the left leg • if the left ventricle increases its activity or its size = left axis deviation • if the right ventricle increases its activity or size = right axis deviation • the overall direction of depolarization is from the right arm to the left leg • if the depolarization wave direction in a lead matches this axis direction = upward deflection in the EKG • Lead III is from left to right = downward deflection
The layout • 4 columns of 3 rows result • each segment is only 1 to 3 heart beats • bottom of the EKG frequently has the rhythm strip – from lead limb II LIMB LEAD I: Right arm -> left arm LIMB LEAD aVR: right arm CHEST LEADS V1-V6 LIMB LEAD II: Right arm -> left leg LIMB LEAD aVL: left arm LIMB LEAD aVF: left leg (foot) LIMB LEAD III: Left arm -> left leg Rhythm strip
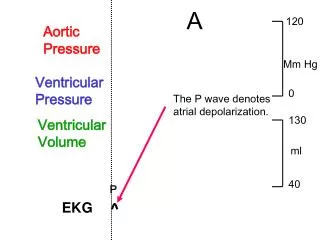
The waves • P wave (80msec) = atrial depolarization • SA to AV node and right atrium to left • absence: atrial fibrillation and SA blocks • increased amplitude = hypokalemia (low K+) • QRS complex (80-120msec) = rapid depolarization of ventricles • problems in Purkinje fibers – widened QRS • used to diagnose: cardiac arrhythmias, conduction abnormalities, ventricular hypertrophy and myocardial infarctions • T wave (160msec) = repolarization of ventricles -last half of T wave = relative refractory or vulnerable period -narrow T wave = hyperkalemia (high K+)
The intervals & segments • PR interval (120-200msec) = SA node through the AV node and into ventricles • indicates AV node function and coordination between atrial and ventricular conduction systems • long interval – 1st degree AV block • PR segment (50-120msec) = end of P wave to the start of the QRS complex • from AV node to the bundles to the Purkinje fibers • essentially the time through the AV node • PR interval is more clinically relevant http://en.wikipedia.org/wiki/File:ECG_principle_slow.gif
The intervals & segments • ST segment (80-120msec) = end of QRS to the start of the T wave -period when ventricles are depolarized • QT interval (up to 420msec) = start of QRS to the end of the T wave • examines the internal conduction of the entire ventricle • prolonged interval is a risk factor for ventricular tachyarrhythmias and sudden death
Other stuff • J point = point at which the QRS finishes and the ST segment begins • used to measure ST elevation or depression • J wave – can appear as a small wave after the QRS • pathogenic – hypothermia and hypocalcemia (low Ca)
Vectors • each lead “views” the heart from different angles and shows which region of the heart is affected • leads II, III and aVF look at electrical activity from the inferior surface of the heart • leads I, aVL, V5 & V6 – from the lateral wall of the left ventricle • leads V1 & V2 – from the septal wall • leads V3 & V4 – from the anterior surface of the heart
Normal EKG • Vertical axis is potential (voltage) • EKG paper has 1 millimeter small squares - so height or depth of wave is measured in millimeters.10 mm = 1.0 mV • Horizontal axis is time. • 40 msec for 1 mm (1 small box). • 200 msec seconds for 1 large box = 5 small boxes = 5 x .04 seconds.
Normal EKG QRS wave = 7-8 mm high in Lead I = 0.7 to 0.8 mV.QRS wave = 0.04 seconds long in Lead I. 10 mm = 1 mV 1 mm = 40 msec 1 large box is 0.5 mV and 200 msec QRS T 7.0mV P 0.04sec 0.5mV 0.2sec
Abnormal EKG Reading Elevated ST
Interpreting the EKG • look at five areas, in order, on each EKG. • Rate • Rhythm (Intervals) • Axis • Hypertrophy • Infarct
Rhythm & Rate • QUESTIONS TO ASK and ANSWER • Are there P waves? • Are they regular? • Does every one precede a QRS? • Is the PR interval constant? • What is the PR interval? • The PR interval should be between 120 and 240 msec (3 to 6 small squares)
Calculating Rate (ventricular rate) -if the QRS lands on a heavy line – count the next as 300
Mathematical method: • official way of determining rate • count the number of boxes between the 1st and 2nd R wave • divide 300 by this number • Use this method if there is a regular bradycardia, i.e. rate < 50. • 7.5 boxes • 300/7.5 large boxes = rate 40.
Six-second method: • Count off 30 large boxes = 6 seconds (remember 1 large box = 0.2 seconds, so 30 large boxes = 6 seconds). • Then, count the number of R-R intervals in six seconds and multiply by 10. • This is the number of beats per minute. • This is most useful if you have an irregular rhythm (like atrial fibrillation) when you want to know an average rate. • There are 8 R-R intervals within 30 boxes. Multiply 8 x 10 = Rate 80.
Rhythm • A reasonable way to group arrhythmias is in four general groups. • 1. Irregular rhythms • 2. Escape & premature beats • 3. Ectopic beats • 4. AV blocks
Rhythm QRS is narrow (normal). If the beat is ventricular in origin, the QRS is wide and bizarre because it doesn't come down the normal pathway. QRS is wide – problem with the Purkinje fibers??
Group 1: Irregular rhythms • A) Sinus arrhythmia. • rate = 45-100 beats/min • this term is used if the rate varies a lot over the strip • P waves and PR intervals are all identical because they originate from the sinus node. • Sinus rate may vary normally a bit (increase with inspiration, decrease with expiration) • inspiration – stretch receptors in lung stimulate cardiac centers in the medulla • QRS is normal • Sinus arrhythmia: P waves are not identical in spacing along the strip.
B) Wandering atrial pacemaker - also called multifocal atrial tachycardia. • different PR intervals – atrial pacemaker shifts locations in the atria • pacemaker shifts from SA node to somewhere in the atria &/or the AV node • increase vagus nerve activity can also cause this – slows the SA node and allows the AV node to take over pacemaker function Flattened P wave or P wave is “notched” Wandering atrial pacemaker - seen best in lead II as flattened or notched P waves
C) Atrial fibrillation: • common arrhythmia. • there are no P waves, only irregular or wavy baseline. • the QRS complexes are irregularly spaced, therefore it is included under irregular rhythms.
Group 2: Escape & Premature beats • escape beat is late • premature beat is early • Atrial escape • Different appearing and late P waves. • Ventricular escape • No P, wide, bizarre QRS.-An ectopic pacemaker fires early before the next scheduled beat. • Premature atrial contraction • "PAC", early and differently shaped P wave, narrow QRS. ventricular escape
Premature ventricular contraction (PVCs) • heartbeat initiated by the Purkinje fibers – feels like palpitations • ventricles contract before the atria – ventricle cannot be filled optimally - No P wave, wide bizarre QRS - PVCs that occur three (3) or more in a row is called ventricular tachycardia (ectopic focus) • numerous causes: drugs (prozac, cocaine), dehydration, hypercalcemia, hypokalemia, stress, heart murmurs, hypoxia, ischemia • treatments – beta-blockers (block the binding of epinephrine & other stress hormones), Ca channel blockers, K+ or Mg+ supplementation PVC PVC PVC
Group 3: Ectopic Focus • excitable group of cells outside of the SA node depolarizes • rate of firing exceeds that of the SA node • if chronic – can lead to tachycardia and fibrillations • [100-250] Tachycardia • [250-350] Flutter • [350+] Fibrillation
Ventricular tachycardia (Vtac): note fast rate and wide bizarre QRS -rapid rhythm originates within the ventricular tissue -absence of P waves -wide bizarre QRS only
Paroxysmal supraventricular tachycardia: • note accelerated rate and narrow QRS complexes • paroxysmal – lasts only a few seconds to a minute – then normal rate and rhythm are re-established • supraventricular – rapid rhythm originates above the ventricular tissue such as the SA node, AV node or from the atrial tissue • treatment – Valsalva maneuver – hold your nose and blow (increase vagal tone) • treatment – cold water on face • treatment – cardiac massage
Atrial flutter: “sawtooth” pattern prior to QRS complexes. Ventricular fibrillation: erratic and wavy baseline.
Group 4: AV blocks 1st degree = AV nodal disease -PR interval > 0.2 seconds (1 large box) - each P is followed by a QRS. - seen also in athletes with increased vagal tone (activity) • can be caused by acute MI, beta-blockers • generally won’t progress • benign condition • but can increase the risk of atrial fibrillation (irregular heartbeat) (occur in three (3) degrees, like skin burns; third degree is the worst). The PR interval is approximately 0.28 seconds.
dropped QRS Type I 2nd degree block or Wenckebach -PR interval gets progressively longer each beat until finally a QRS is "dropped" (missing). -a pattern in the dropping can be discerned -disease of the AV node
Type 2 - 2nd degree block or Mobitz -PR intervals are constant and a QRS is "dropped" intermittently. -BUT no pattern in the dropping can be discerned -disease of the Bundles of His and Purkinje fibers Dropped QRS P wave Dropped QRS P wave Normal PR interval
P P P P • 3rd degree block • The atrial rate is independent of the ventricular rate (P wave and QRS appearances are not related). • The clue here is no relationship at all of the P-R intervals. • The P-R interval is constantly changing, the QRS is usually wide and bizarre because it is ventricular origin.
Bundle Branch Blocks • Right bundle branch block occurs as a congenital anomaly or is associated with volume overload in the right ventricle. • Left bundle branch block is almost always pathological, reflecting disease of the left ventricle.
EKG lab: in class lab 300 150 100 75
Estimate the rhythm of this strip Is the pattern normal? What condition is this??
Is the pattern normal? What atrial condition is this??
Look at the P waves – are they normal? What atrial condition is this??
This condition lasts only a few seconds what is it?