Download
1 / 26
260 likes | 325 Views
This topic explores the biological bases of behavior, focusing on the control of movement through skeletal muscles. It delves into the anatomy of skeletal muscle fibers, the neuromuscular junction, smooth and cardiac muscle behavior, muscle sensory feedback mechanisms, spinal cord anatomy, and cortical control of movement. Key concepts include muscle twitch, motor unit size, neuromuscular junction neurotransmitters, muscle sensory receptors, spinal reflexes, and the role of different brain regions in motor control. Explore the intricate mechanisms involved in orchestrating movements in the human body.

E N D
Biological Bases of Behavior 8: Control of Movement m d
Skeletal Muscle • Movements of our body are accomplished by contraction of the skeletal muscles • Flexion: contraction of a flexor muscle draws in a limb • Extension: contraction of extensor muscle • Skeletal muscle fibers have a striated appearance • Skeletal muscle is composed of two fiber types: • Extrafusal: innervated by alpha-motoneurons from the spinal cord: exert force • Intrafusal: sensory fibers that detect stretch of the muscle • Afferent fibers: report length of intrafusal: when stretched, the fibers stimulate the alpha-neuron that innervates the muscle fiber: maintains muscle tone • Efferent fibers: contraction adjusts sensitivity of afferent fibers. 8.2
Each muscle fiber consists of a bundle of myofibrils Each myofibril is made up of overlapping strands of actin and myosin During a muscle twitch, the myosin filaments move relative to the actin filaments, thereby shortening the muscle fiber Skeletal Muscle Anatomy 8.3
Neuromuscular Junction • The neuromuscular junction is the synapse formed between an alpha motor neuron axon and a muscle fiber • Each axon can form synapses with several muscle fibers (forming a motor unit) • The precision of muscle control is related to motor unit size • Small: precise movements of the hand • Large: movements of the leg • ACh is the neuromuscular junction neurotransmitter • Release of ACh produces a large endplate potential • Always cause muscle fiber to fire • Voltage changes open CA++ channels • CA++ entry triggers myosin-actin interaction (rowing action) • CA++ as a cofactor that permits the myofibrils to extract energy from ATP • Movement of myosin bridges shortens muscle fiber 8.4
Smooth and Cardiac Muscle • Smooth muscle is controlled by the autonomic nervous system • Multiunit smooth muscle is normally inactive • Located in large arteries, around hair and in the eye • Responds to neural or hormonal stimulation • Single-unit smooth muscle exhibits rhythmic contraction • Muscle fibers produce spontaneous pacemaker potentials that elicit action potentials in adjacent smooth muscle fibers • Single-unit muscle is found in gastrointestinal tract, uterus, small blood vessels • Cardiac muscle fibers resemble striated muscle in appearance, but exhibit rhythmic contractions like that of single-unit smooth muscle 8.5
Muscle Sensory Feedback • Striated muscle contraction is governed by sensory feedback • Intrafusal fibers are in parallel with extrafusal fibers • Intrafusal receptors fire when the extrafusal muscle fibers lengthen (load on muscle) • Actually detect the length of muscle • Intrafusal fibers activate agonist muscle fibers and inhibit antagonist muscle fibers • Extrafusal contraction eliminates intrafusal firing • Golgi tendon organ (GTO) receptors are located within tendons • Sense degree of stretch on muscle • GTO activation inhibits the agonist muscle (via release of glycine onto alpha-motoneuron • GTO receptors function to prevent over-contraction of striated muscle 8.6
Spinal Cord Anatomy • Spinal cord is organized into dorsal and ventral aspects • Dorsal horn receives incoming sensory information • Ventral horn issues efferent fibers (alpha-motoneurons) that innervate extrafusal fibers 8.7
Spinal Cord Reflexes • Monosynaptic reflexes involve a single synapse between a sensory fiber from a muscle and an alpha-motor neuron • Sensory fiber activation quickly activates the alpha motor neuron which contracts muscle fibers • Patellar reflex • Monosynaptic stretch reflex in posture control • Polysynaptic reflexes involve multiple synapses between sensory axons, interneurons, and motor neurons • Axons from the afferent muscle spindles can synapse onto • Alpha motoneuron connected to the agonist muscle • An inhibitory interneuron connected to the antagonist muscle • Signals from the muscle spindle activate the agonist and inhibit the antagonist muscle 8.8
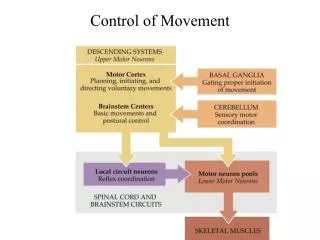
Motor Cortex • Multiple motor systems control body movements • Walking, talking, postural, arm and finger movements • Primary motor cortex is located on the precentral gyrus • Motor cortex is somatotopically organized (motor homunculus) • Motor cortex receives input from • Premotor cortex • Supplemental motor area • Frontal association cortex • Primary somatosensory cortex • Planning of movements involves the premotor cortex and the supplemental motor area which influence the primary motor cortex 8.10
Motor “Homunculus” 8.11
Descending Motor Pathways • Axons from primary motor cortex descend to the spinal cord via two groups • Lateral group: controls independent limb movements • Corticospinal tract: hand/finger movements • Corticobulbar tract: movements of face, neck, tongue, eye • Rubrospinal tract: fore- and hind-limb muscles • Ventromedial group control gross limb movements • Vestibulospinal tract: control of posture • Tectospinal tract: coordinate eye and head/trunk movements • Reticulospinal tract: walking, sneezing, muscle tone • Ventral corticospinal tract: muscles of upper leg/trunk 8.17
Corticospinal Tract • Neurons of the corticospinal tract terminate on motor neurons within the gray matter of the spinal cord • Corticospinal tract starts in layer 5 of primary motor cortex • Passes through the cerebral peduncles of the midbrain • Corticospinal neurons decussate (crossover ) in the medulla • 80% become the lat. corticospinal tract • 20% become the ventral corticospinal tract • Terminate onto internuncial neurons or alpha-motoneurons of ventral horn • Corticospinal tracts control fine movements • Destruction: loss of muscle strength, reduced dexterity of hands and fingers • No effect of corticospinal lesions on posture or use of limbs for reaching 8.18
The Apraxias • Apraxia refers to an inability to properly execute a learned skilled movement following brain damage • Limb apraxia involves movement of the wrong portion of a limb, incorrect movement of the correct limb part, or an incorrect sequence of movements • Callosal apraxia: person cannot perform movement of left hand to a verbal request (anterior callosum interruption prevents information from reaching right hemisphere) • Sympathetic apraxia: damage to anterior left hemisphere causes apraxia of the left arm (as well as paralysis of right arm and hand) • Left parietal apraxia: difficulty in initiating movements to verbal request • Constructional apraxia is caused by right parietal lobe damage • Person has difficulty with drawing pictures or assembling objects 8.19
The Basal Ganglia • Basal ganglia consist of the caudate nucleus, the putamen and the globus pallidus • Input to the basal ganglia is from the primary motor cortex and the substantia nigra • Output of the basal ganglia is to • Primary motor cortex, supplemental motor area, premotor cortex • Brainstem motor nuclei (ventromedial pathways) • Cortical-basal ganglia loop • Frontal, parietal, temporal cortex send axons to caudate/putamen • Caudate/putamen projects to the globus pallidus • Globus pallidus projects back to motor cortex via thalamic nuclei 8.20
Parkinson’s Disease • Parkinson’s disease (PD)involves muscle rigidity, resting tremor, slow movements • Parkinson’s results from damage to dopamine neurons within the nigrostriatal bundle (projects to caudate and putamen) • Slow movements and postural problems result from • Loss of excitatory input to the direct circuit (caudate-Gpi-VA/VL thalamus-motor cortex) • Loss of output from the indirect circuit (which is overall an excitatory circuit for motor behavior) • Neurological treatments for PD: • Transplants of dopamine-secreting neurons (fetal subtantia nigra cells or cells from the carotid body) • Stereotaxic lesions of the globus pallidus (internal division) alleviates some symptoms of Parkinson’s disease • Electrode implants 8.22
Parkinson’s Disease 8.23
Parkinson’s Disease 8.24
Huntington’s Disease • Huntington’s disease (HD)involves uncontrollable, jerky movements of the limbs • HD is caused by degeneration of the caudate nucleus and putamen • Cell loss involves GABA-secreting axons that innervate the external division of the globus pallidus (GPe) • The GPe cells increase their activity, which inhibits the activity of the subthalamic nucleus, which reduces the activity level of the GPi, resulting in excessive movements • HD is a hereditary disorder caused by a dominant gene on chromosome 4 • This gene produces a faulty version of the protein huntingtin 8.25
The Cerebellum • Cerebellum consists of two hemispheres with associated deep nuclei • Flocculonodular lobe is located at the caudal aspect of the cerebellum • This lobe has inputs and outputs to the vestibular system • Involved in control of posture • Vermis is located on the midline of the cerebellum • Receives auditory and visual information from the tectum and cutaneous information from the spinal cord • Vermis projects to the fastigial nucleus which in turn projects to the vestibular nucleus and to brainstem motor nuclei • Damage to the cerebellum generally results in jerky, erratic and uncoordinated movements 8.26