Download
1 / 27
270 likes | 701 Views
ECMO application : ruled implementation or free diffusion?. Milan 2012 Palle Palmér ECMO Centrum Karolinska Karolinska University Hospital, Stockholm Sweden. If we look at Stockholm development. ECMO is a simple technic. But not that simple You need to know a lot of

E N D
ECMO application:ruled implementation or free diffusion? Milan 2012 Palle Palmér ECMO Centrum Karolinska Karolinska University Hospital, Stockholm Sweden
ECMO is a simple technic • But not that simple • You need to know a lot of • Cannulas, oxygenators, oxygen delivery and consumption, carbon oxide, coagulation • Interrelation between ECMO circuit, the ventilator and the CVVHDF machine • The doctor and nurses in charge has to know this 24/7 4 ECMO Centrum Karolinska
One doctor has to be totally responsible • The week has 168 hours • In Saturday morning at 4 am you have to have one experienced doctor to handle problems. • It not enough with one interested doctor in the ward daytime for 40 hours a week. At least he/she has to be dedicated to come in the other 128 hours too. • ECMO is not run by itself for 128 hours a week. 5 ECMO Centrum Karolinska
We have to make a different between Cardiac and Respiratory ECMO • Cardiac ECMO should probably be done in all thoracic surgical departments. • Most of these patients comes from the operation table and need a short term assistance. • If the patient get a lung edema it will be complicated and take much more time. 6 ECMO Centrum Karolinska
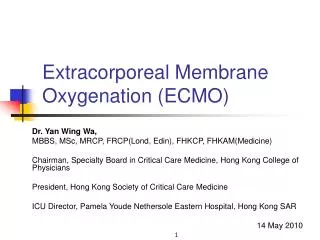
Multistagecannulae v.cava.suplowsaturation v.cava.inf high saturation MRI Jonas A Lindholm
Respiratory ECMO • Needs volume and centralization • Long run ECMO 15- 60 days • Much more maintenance – circuit change and clotting problems • Totally whiteout lungs makes the safety marginal to 30 seconds • Low saturation • How to ventilate 8 ECMO Centrum Karolinska
Burn patient consuming 450 ml of oxygen per minute 9 ECMO Centrum Karolinska
68 days run with saturation of 65% in 45 days 10 ECMO Centrum Karolinska
Multi-Organ-failure • Decreased urine output • Increasing liver values • Low blood pressure • RIGHT SIDED HEART FAILURE - Convert to V-A ECMO • Hemolysis – clotting in the circuit - Solve that problem 11 ECMO Centrum Karolinska
Does volume make different ? • In a low volume unit less then 10 patient per year , less then 150 days per year, you need much more assistance from perfusionists. • It will be more expensive • Lack of perfusion capacity for the operation • Lack of beds in the thoracic intensive care • Less persistence 12 ECMO Centrum Karolinska
In normal or thoracical ICU • High volume center, at least one ECMO case every day of the year in the ward. It’s a normal part of the ICU treatment. • The safety will be in the walls due to dedicated nurses and doctors experience. • Much more persistence. • Possible to have the patients awake. • Possible to learn how to solve problems. 13 ECMO Centrum Karolinska
ELSO reports July 2012 14 ECMO Centrum Karolinska
The big well developed ECMOcenters • Reports survival rate of 70-80%, Stockholm and Leicester, even with mean p/F ratios of 50 and 65. • That means that the smaller centers have an survival rate of about 50% • It´s also possible that the experience centers takes more odd cases. 15 ECMO Centrum Karolinska
Mean p/f ratio 1995 – 2008 2008 1995
A new indicationSepticshock • SAPPS III scoring 2012 • 10 patient with septic shock mean 80 points • Mortality risk of 85% • Low leucocytes declining to < 2 ”ALARM ALERT” • Inotropic index > 100 • Cold sepsis in some of them - amputation • Survival rate 80% • V-A ECMO because of cardiogenic shock
Trauma is an undeveloped field • No heparin untilthey stop bleeding • The Problem is that the major trauma casesdon’tdiewithin 1-2 hours. • Theyare still alive 10 hours later, and weempty the blood bank,and the surgeonsaretired • Youcan pack the thoraciccavity, to stop bleedings 18 ECMO Centrum Karolinska
10 million people per ECMO center • You will have respiratory ECMO • 40 -50 adult patient per year mean 15 days ( 7-60 days) • 30-40 pediatric patient mean 15 days ( 7-60 days) • 30-40 neonates mean 7 days ( 4-30 days) • You need an ECMO transport organization that can transport 24/7 19 ECMO Centrum Karolinska
An high volume center • Can take the full advantage of the ECMO circuit • The goal is not to come off the machine • The goal is to have a healthy patient 20 ECMO Centrum Karolinska
Pneumothorax • Don’t hurt the patient • First choice - stop ventilation in 2-3 days • Pleura drainage - Seldinger or Surgeon 21 ECMO Centrum Karolinska
A very small pleuradrainage - 20 liter of blood and 4 operations 22 ECMO Centrum Karolinska
Maybe we should look at survival as something obvious • Why did they die and was it preventable • Last 2 years 78 adult patient Sapps III mortality rate of 85% • 17 patient died (22%) • 5 patient we didn´t have a chance from beginning • 5 patient in pseudomonas and fungus • 4 intracranial bleeding septic embolus pre ECMO • 3 intracranial bleeding due to the ECMO treatment 23 ECMO Centrum Karolinska
When you look at the pump and as your best friend then you are a mature ECMO unit • Learn everything about the • pump oxygenators tubings and cannulaes • Train,train,train • Be careful • Be patient • Be trained • Don’t solve problems that doesn’t have to be solved
EURO-ELSO 2013 Precongress 8-9 May 2013 Congress 9-11 May 2013 Scientificprogramme Nov 2012 Deadline for Abstracts 15 March 2013