Download
1 / 26
260 likes | 443 Views
The Shoulder = glenohumeral jt. The glenohumeral joint is a ball-and-socket joint that allows for the arm to move in a circular rotation as well as movement of the arm towards and away from the body. The motion that the glenohumeral joint provides is flexion, extension, abduction and adduction.

E N D
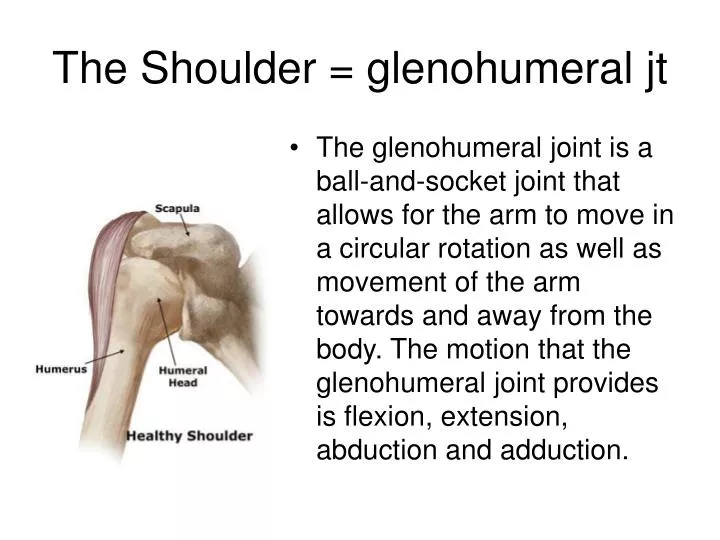
The Shoulder = glenohumeral jt • The glenohumeral joint is a ball-and-socket joint that allows for the arm to move in a circular rotation as well as movement of the arm towards and away from the body. The motion that the glenohumeral joint provides is flexion, extension, abduction and adduction.
In Anatomical Position, the head of the humerus is medial, slightly posterior and superior in the glenoid fossa. While the glenoid cavity faces laterally forward and superior.
Acromioclavicular Joint (AC joint) • a gliding joint within the shoulder. This joint is specific to primates and humans, allowing for the ability to raise the arm above the head. This joint functions as a pivot point, acting like a strut to help with movement of the scapula resulting in a greater degree of arm rotation. Also, the AV joint allows for the transmission of force from the upper arm to the rest of the skeleton
The AV joint is formed between the clavicle and the scapula. The acromion, a section of the scapula, is the binding site for the clavicle. These two bones fit together, but are not stable on their own. Ligaments & muscles are used to stabilize the AV joint. Two sets of muscles are important for the stabilization of this joint in the proper joint formation. [ help stabilize the clavicle and the scapula] 1) the trapezius: The upper trapezius muscle fibers connects the lower base of the skull to the clavicle. The middle and lower trapezius muscle fibers connect vertebrae in the spine to the scapula. 2) the deltoid: The anterior deltoid connects the clavicle to the humerus, while the posterior and lateral deltoid fibers connect the scapula to the humerus.
Trapezius • Large superficial, flat triangular muscle of upper back. Originates on the occipital bone of skull, ligamentum nuchae and 7 cervical and all thoracic vertebrae and inserts onto the clavicle, acromion and spine of the scapula. • Because the fibers run in different directions, it has a variety of actions. Different fibers control different actions: • The superior (upper) fibers elevate the scapula: scapular elevation (shrugging up), • the middle fibers retract it: scapular adduction (drawing the shoulder blades together) • The inferior (lower) fibers depress it: depression (pulling the shoulder blades down) • When the superior and inferior fibers act together they superiorly (upwardly) rotate the scapula.
Deltoids • forms the rounded contour of the human shoulder.
Origin • It arises in three distinct sets of fibers • Anterior fibers: from the anterior border and upper surface of the lateral third of the clavicle • Middle fibers: from the lateral margin and upper surface of the acromion. • Posterior fibers: from the lower lip of the posterior border of the spine of the scapula, as far back as the triangular surface at its medial end
Insertion • All the fibers converge, the middle passing vertically, the anterior obliquely backward and lateralward, the posterior obliquely forward and lateralward; • they unite in a thick tendon, which is inserted into the V-shaped deltoid tubercle on the middle of the lateral aspect of the shaft of the humerus.
Action • The anterior fibers: shoulder abduction when the shoulder is externally rotated. • The posterior fibers: involved in transverse extension. The posterior deltoid is also the primary shoulder hyperextensor. • The lateral fibers: shoulder abduction when the shoulder is internally rotated, are involved in shoulder flexion when the shoulder is internally rotated, and are involved in shoulder transverse abduction (shoulder externally rotated) -- but are not utilized significantly during strict transverse extension (shoulder internally rotated).
Rotator Cuff an anatomical term given to the group of muscles & their tendons that act to stabilize the shoulder.
Function of Rotator Cuff hold the head of the humerus in the small and shallow glenoid fossa of the scapula. During elevation of the arm, the rotator cuff compresses the glenohumeral joint in order to allow the large deltoid muscle to further elevate the arm. In other words, without the rotator cuff, the humeral head would ride up partially out of the glenoid fossa and the efficiency of the deltoid muscle would be much less.
Muscles comprising rotator cuff • Supraspinatus • Infraspinatus • Teres Minor • Subscapularis • A mnemonic to remember what muscles form the rotator cuff is SITS (supraspinatus, infraspinatus, teres minor, subscapularis)
Rotator Cuff Injury • injury to 1 or more of the 4 muscles in the shoulder. This shoulder injury may come on suddenly and be associated with a specific injury such as a fall (acute), or it may be something that gets progressively worse over time with activity that aggravates the muscle(s) (chronic). • can range from an inflammation of the muscle without any permanent damage, such as tendinitis, to a complete or partial tear of the muscle that might require surgery to fix it.
Chronic tear • Found among people in occupations or sports requiring excessive overhead activity (examples: painters, baseball pitchers) • Variations in the shoulder structure causing narrowing under the outer edge of the collarbone
Symptoms • Occur more often in a person's dominant arm • More commonly found among men older than 40 years • Pain usually worse at night and interferes with sleep • Worsening pain followed by gradual weakness • Decrease in ability to move the arm, especially out to the side • Able to use arm for most activities but unable to use the injured arm for activities that entail lifting the arm as high or higher than the shoulder to the front or side
Acute tear • Sudden powerful raising of the arm against resistance, often in an attempt to cushion a fall (examples: heavy lifting, a fall on the shoulder) • Injury usually associated with a significant amount of force if person is younger than 30 years
Symptoms • Sudden tearing sensation followed by severe pain shooting through the arm • Motion limited by pain and muscle spasm • Acute pain from bleeding and muscle spasm (often goes away in a few days) • Point tenderness over the site of rupture • With large tears, inability to raise the arm out to the side, although this can be done with help
Tendinitis • Degeneration (wearing out) of the muscles with age • Repetitive trauma to the muscle by everyday movement of the shoulder
Symptoms • More common in women aged 35-50 years • Deep ache in the shoulder also felt on the outside upper arm • Point tenderness • Pain comes on gradually and becomes worse with lifting the arm to the side or turning it inward • May lead to a chronic tear
When to call the doctor • If shoulder pain lasts more than 2 days • If shoulder problems (pain) do not allow you to work • If you are unable to reach overhead to get an item in a cabinet above shoulder level, for example • If you are unable to play a certain sport such as baseball or engage in an activity such as swimming
When to go to the hospital • For any acute injury in which you are unable to move the injured shoulder as well as the uninjured shoulder, seek emergency medical care.