Download

1 / 22
220 likes | 250 Views
Detailed insight into the Texas Children’s Hospital conversion project, managing tenants, infrastructure challenges, and relationship building in the community.

E N D
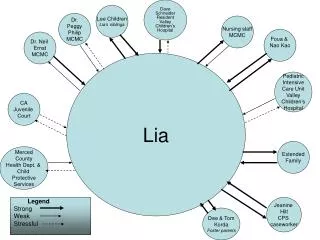
2 TEXAS CHILDREN’S HOSPITAL
TCH Conversion $6.6M – Initial Construction Budget (10% Contingency Included) $6.6M – Actual Construction Budget $13 M – Overall Approved Project Budget $12.6M – Actual Total Commitment To Project Building Relationships with Community – Metro, Local Council Managing non-TCH tenants (Dental) – infrastructure heavy & delayed opening timing
TCH MEDICAL HOME PEDI PATIENT PROCESS MODEL - 01/30/2012 EXAM VISIT HISTORY & PHYSICAL TIME BASED ON ESTABLISHED PT HISTORICAL DISTRIBUTION 5-40 MINS ARRIVAL AT MEDICAL HOME PT TAKEN TO EXAM ROOM VITALS TAKEN ON WAY LAB DRAW AR VITALS IF REQ 3-5 MINS DISCHARGE IN EXAM ROOM UNLESS COMPLEX DISCHARD NEEDED 3-10 MINS SICK VISIT DISCOVERY OF ISSUE PATIENT LEAVE MEDICAL HOME PT TO SUB WAITING FOR NAVIGATOR GATHERS ANY SIGNITURES AND REVIEWS NECESSARY DOCUMENTS CHECK-IN KIOSKS FOR ESTABLISHED PATIENTS? 3-5 MINS TO TREATMENT ROOM 20-90 MINS TO COMPLEX DISCHARGE AREA FOR SCHEDULING DIAG OR TREATMENT 10-20 MINS SICK CHILD WELL VISIT NEW VISIT %$ WELL VS. SICK EXAM VISIT HISTORY & PHYSICAL TIME BASED ON ESTABLISHED PT HISTORICAL DISTRIBUTION 5-40 MINS PT TAKEN TO EXAM ROOM VITALS TAKEN ON WAY 3-5 MINS DISCHARGE IN EXAM ROOM UNLESS COMPLEX DISCHARD NEEDED 3-10 MINS WELL VISIT DISCOVERY OF ISSUE PATIENT LEAVE MEDICAL HOME TO COMPLEX DISCHARGE AREA FOR SCHEDULING DIAG OR TREATMENT 10-20 MINS EXAM VISIT HISTORY & PHYSICAL TIME BASED ON ESTABLISHED PT HISTORICAL DISTRIBUTION 10-60 MINS PT TAKEN TO EXAM ROOM VITALS TAKEN ON WAY 3-5 MINS NEW VISIT DID WE WANT TO MODEL PATIENTS HAVING THEIR PERSCRIPTIONS BROUGHT TO THEM IN THE EXAM ROOM, OR WAITING IN A SUB-WAITING AREA? THIS SIMPLIFIED FLOW DIAGRAM IS USEFUL TO LOOK AT THE NUMBER OF EXAM ROOMS IN A STANDARD CARE TRACK. HOW WITH THIS FLOW DIFFER FOR PED PATIENTS IN A CENTERING CONCEPT? WHAT % OF PATIENTS COULD THIS BE?
Site Selection Reflects Pilot Program Preferred Area • Membership Density • Proximity To Potential Partner Hospitals • Near Major Freeways site TMC CBD
Vehicular Access • Site Along Beltway Feeder Road • Can Be Approached From Multiple Directions I 45 N B 8
TCH Medical Home Existing Building
Site Organization 1 1 4 2 3 6 2 5 6 Parking • 1=Patient & Public Parking • Staff Parking • Patient Flow from Bus Stop • Main Entry • Public Retail Entry • Staff Entry N
Public Areas • Main Entry/Drop-Off • Public Retail Entry • North/East Natural Light • Waiting/Circulation • Retail Corridor 3 a 1 a 3 4 2
Program Plan 10 13 3 Public/Retail/EDU/Admin • Main Entry/Drop-Off • Public Retail Entry • Waiting/Circulation • Retail Corridor • Pharmacy • Dental • Optometry • Education • Administration Staff • Staff Work Area OB Program Space • OB Clinic • Centering Peds Program Space • Primary Care Clinic • Specialty Clinic • Diagnostics a 1 14 a 15 3 7 5 12 8 11 9 4 6 11 2 10
TCH Medical Home Reception
TCH Medical Home Waiting
TCH Medical Home Team Workstations
TCH Medical Home Reception
3 Lessons Learned
POE Methodology (to be provided at learning session)
POE Results (to be provided at learning session)
Large, open footplate Opportunity for various ceiling heights / high ceilings Potential for second floor / mezzanine Opportunity for skylights Potential for separate front-of-house and back-of-house Good visibility from major thoroughfares Ample parking Economical investment Places care directly in the target community Create a feeder system to or away from hospital campus Common Takeaways – Conversion “Pros”
Inappropriate column spacing Undersized / shared utilities with adjoining tenants Usually no emergency generators Inappropriate / unusable mechanical systems Low-budget original construction Poorly documented building alterations over time Undocumented / undiscoverable existing conditions Potential limitations to exterior façade changes Significant saw-cutting for under-floor plumbing High roof: ceiling-mounted equipment challenging Security Common Takeaways - Conversion “Cons”
Dianna Prachyl DPrachyl@jpshealth.org JPS Allison Muth ABMuth@texaschildrens.org TCH Diane Osan DOsan@fkp.com FKP Lance Winn LWinn@fkp.com