Download
1 / 61
610 likes | 803 Views
Diabetes - Overview. Veronica Piziak MD, PhD Endocrinology, Scott & White. Disclosures: Research support: J&J . Objectives: Discuss: Diagnosis of diabetes Treatment goals Incorporating new medications into practice Inpatient management of diabetes Pump use Hyperosmolar state.

E N D
Diabetes - Overview Veronica Piziak MD, PhD Endocrinology, Scott & White
Disclosures:Research support: J&J Objectives: Discuss: Diagnosis of diabetes Treatment goals Incorporating new medications into practice Inpatient management of diabetes Pump use Hyperosmolar state
Type 2 DiabetesDefinition • A disorder of glucose, lipid, protein metabolism characterized by peripheral insulin resistance, inadequate pancreatic insulin secretory response and disordered glucagon supression. • Risk factors: • Obesity • Heredity • Environment
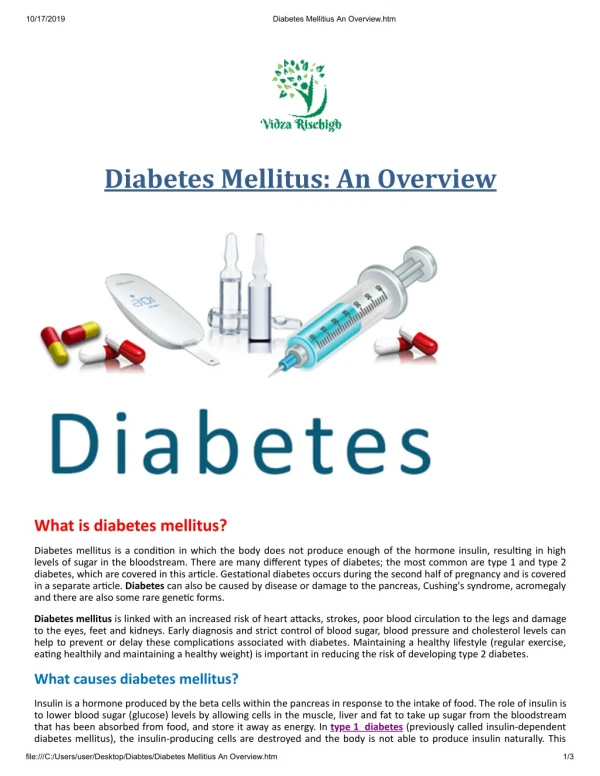
<22 <23 23-23.9 24-24.9 25-26.9 27-28.9 29-30.9 31-32.9 33-34.9 35+ Relationship Between BMI and Risk of Type 2 Diabetes 93.2 Men Women 54.0 Age-Adjusted Relative Risk 42.1 40.3 27.6 21.3 15.8 8.1 5.0 11.6 4.3 2.9 2.2 6.7 4.4 1.5 1.0 1.0 1.0 Body Mass index (kg/m2) Chan J et al. Diabetes Care 1994;17:961. Colditz G et al. Ann Intern Med 1995;122:481.
Obesity Trends Among U.S. Adults 2009 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30% CDC Data 2010
County-level Estimates of Diagnosed Diabetes forAdults aged ≥ 20 years: United States 2008 Metabolic syndrome
NCEP ATP III: Working Definition of the Metabolic Syndrome 3 of the following: Risk Factor Defining Level Abdominal obesity (waist circumference*) Men Intramesenteric Fat >102 cm (>40 in) Women > 88 cm (>35 in) Triglycerides 150 mg/dL HDL cholesterol Men <40 mg/dL Women <50 mg/dL Blood pressure 130/85 mm Hg Fasting glucose 100 mg/dL *Some male patients may develop multiple metabolic risk factors when waist circumference is only marginally increased (eg, 94–102 cm [37–40 inches]). NCEP ATP III. JAMA. 2001;285:2486–2495.
Food Plan for Metabolic Syndrome, Prediabetes, Type 2 Diabetes • Caloric restriction is the key • Low CHO (6-8) with monounstaurated fats decreases insulin resistance • High complex CHO and fiber (25 gm) decrease insulin resistance • Fresh fruits and vegetables are important. Lara-Castro C et al 2004 JCE&M;89:4197 • Meal replacements work! • Add 150 minutes of exercise / week
When to use metformin for prevention • In addition to lifestyle counseling, metformin may be considered in those who are at very high risk for developing diabetes (combined IFG and IGT plus other risk factors such as A1C >6%, hypertension, low HDL cholesterol, elevated triglycerides, or family history of diabetes in a first-degree relative) and who are obese and under 60 years of age. • ADA practice guidelines 2010
Diagnosis of Diabetes • A1c may now be used • Prediabetes 5.7 - 6.4% • Diabetes 6.5% • Laboratory determination, venous sample • Not point of care testing • ADA practice guidelines 2010
(mg/dL) 8.5 Diabetes 7.5 126 IFG IFG + IGT 6.5 100 Fasting Glucose (mmol/L) Normal glucose IGT 5.5 4.5 3.5 2.5 4.5 6.5 8.5 10.5 12.5 14.5 7.0 11.1 140 200 (mg/dL) 2-h Postload Glucose (mmol/L) Diagnostic Criteria for Diabetes, IFG, and IGT IFG = impaired fasting glucose. American Diabetes Association. Diabetes Care. 2003;26(suppl 1):S5-S20.
Hyperglycemia Hypertension Dyslipidemia ADA Treatment Goals American Diabetes Association. Diabetes Care. 2010
ADA RENAL GUIDELINES • MICROALBUMIN/CREATININE SPOT URINE ANNUAL SCREENING • ANNUAL CREATININE • ESTIMATE GFR TO CHECK FOR DISEASE • www.kidney.org/professionals/kdoqi/gfr_ calculator.cfm • NEED AGE,GENDER,CREATININE,RACE
STATIN IN DIABETES • CONTROL OF: LIPIDS LDL < 100 (<70) > Age 40 Statins recommended regardless of LDL Reduce the LDL by 30- 40% ADA Practice Guidelines Jan 2010 Diabetes Care Statins are contraindicated in pregnancy Aspirin in any diabetic who has had a CV event and men> 50, women >60 with a risk factor
The Goals of Glucose Control in Type 2 Diabetes Depend on the patient and the duration of disease
Conventional Monotherapies are Unable to Maintain Glycemic Control Over Time United Kingdom Prospective Diabetes Study (UKPDS) 10 Duration of disease Conventional* 9 Insulin Glibenclamide (glyburide) 8 MET Median A1C (%) ADA Goal 7 AACE Goal 6 0 0 3 6 9 12 15 Time from randomization (years) *Conventional therapy defined as dietary advice given at 3-month intervals where FPG was targeted at best levels feasible in clinical practice. If FPG exceeded 270 mg/dL, patients were re-randomized to receive nonintensive MET, chlorpropamide, glibenclamide, or insulin. If FPG exceeded 270 mg/dL again, those on SU would have MET added. If FPG exceeded 270 mg/dL after this, insulin was substituted. MET = metformin; SU = sulfonylurea; FPG = fasting plasma glucose Adapted from UK Prospective Diabetes Study (UKPDS 34) Group. Lancet. 1998;352:854–865.
UKPDSStudy Results: Legacy Effect of Early Glucose Control (Ins/SU Cohort) After median 8.5 years’ post-trial follow-up 1997 2007 * P values were calculated with the use of the log-rank test. RRR=relative risk reduction; SU=sulfonylurea. Diabetes Trials Unit. UKPDS Post Trial Monitoring. UKPDS 80 Slide Set. Available at: http://www.dtu.ox.ac.uk/index.php?maindoc=/ukpds/. Accessed 12 September, 2008. Holman RR, et al. N Engl J Med. 2008;359:epub ahead of print.
Action to Control CardiOvascular Risk in DiabetesACCORD Update • On February 6, 2008, NHLBI announced they have decided to stop the intensive glycemic treatment arm of the trial • Per DSMB scheduled review • Higher incidence of deaths in the intensive treatment group (HbA1c <6.0%) vs the standard treatment group (HbA1c 7.0% to 7.9%) • Death rates in both glycemic control groups were lower than seen in similar populations in other studies
ACCORD • Adverse events • Hypoglycemia no. (%) I S • Requiring medical assistance 538 (10.5) 179 (3.5) <0.001 • Requiring any assistance 830 (16.2) 261 (5.1) <0.001 • Fluid retention — no./total no. (%)‡ 3541/5053 (70.1) 3378/5054 (66.8) <0.001 • Clinical measures • Weight gain >10 kg since baseline — no./total no. (%) 1399/5036 (27.8) 713/5042 (14.1) <0.001 • NEJM June 12, 2008 vol. 358 no. 24 • Effects of Intensive Glucose Lowering in Type 2 Diabetes
Does intensive glucose control prevent death? • Meta analysis of data from 5 clinical trials involving 27,802 adults with Type 2 diabetes • VADT,ACCORD,ADVANCE,UKPDS (2) • 5 year risk of MI, Stroke, CHF, CV death, all cause mortality • No reduction in fatality ,CHF, Stroke • Significant increase in hypoglycemia • Kelly TN Ann Inter Med 2009;151:394-403
How Low should we go? • Early aggressive therapy • <7.0 if possible without hypoglycemia ADA Guidelines Goals of therapy: • Control glucose – individual level for patient • HbA1c 7-7.5% for patients with multiple • comorbidities ?? Avoid hypoglycemia! • Prevent microvascular complications • Prevent macrovascular complications • Montori VM, Fernandez-Balsells ann Int Med 2009;150:803-808
Intensive vs Conventional Glucose Control in Critically Ill PatientsThe NICE-SUGAR Investigators • 3000 patients completed in each arm, groups well matched • Methods Within 24 hours after admission to an intensive care unit (ICU), adults were randomly assigned to undergo either intensive glucose control, target blood glucose range of 81 to 108 mg% • conventional glucose control, with a target of 180 mg% or less • The primary end point as death from any cause within 90 days after randomization. • 2009 NEJM;360:1283
NICE-SUGAR Study • Results: A total of 829 patients (27.5%) in the intensive-control group and 751 (24.9%) in the conventional-control group died (odds ratio for intensive control, 1.14, 95% confidence interval, 1.02 to 1.28; P=0.02). • Operative (surgical) patients and nonoperative (medical) patients (odds ratio for death in the intensive-control group, 1.31 and 1.07, respectively; P=0.10). NS • Severe hypoglycemia (blood glucose level, 40 mg per deciliter was reported in 206 of 3016 patients (6.8%) in the intensive-controlgroup and 15 of 3014 (0.5%) in the conventional-control group (P<0.001). • There was no significant difference between the two treatment groups in the median number of days in the ICU (P=0.84) or hospital (P=0.86) or the median number of days of mechanical ventilation (P=0.56) or renal-replacement therapy (P=0.39). • Conclusion: Blood glucose target of less than 180 mg% resulted in lower mortality than a target of 81 to 108 mg%. On the basis of our results, we do not recommend use of the lower target in critically ill adults. • Check Mayo Clinic Proceedings May 2009;84:400
Treating Diabetes: Insulin resistance Beta and Alpha Cell Dysfunction
Antidiabetic agents: Mechanism of Action 2 Muscle and adipose tissue: glucose uptake/ glucose utilization Metformin, TZDs 1 Intestine: glucose/Fat absorptiondecreased digestion of carbohydrate/fat– Acarbose/ Xenical, bile acid binding resin Insulin resistance TZD’s preserve Beta cell function Blood glucose 4 Liver: hepatic glucose output Metformin HGO Insulinresistance 3Pancreas: insulin secretion Sulfonylureas, nateglinide DeFronzo RA. Diabetes. 1988;37:667-687.Lebovitz HE. In Joslin's Diabetes Mellitus. 1994:508-529; Amatruda JM. In: Diabetes Mellitus. 1996. DeFronzo RA et al. J Clin Endocrinol Metab. 1991;73:1294-1301. Whitcomb RW et al. In: Diabetes Mellitus. 1996;Cavaghan MK et al. J Clin Invest. 1997;100:530-537.Ehrmann DA et al. J Clin Endocrinol Metab. 1997;82:2108-2116; Wolffenbuttel BHR. Eur J Clin Pharmacol. 1993;45:113-116
Upon ingestion of food… GLP-1 Modes of Action in Humans • Stimulates glucose-dependent insulin secretion • Suppress glucagon secretion • Slows gastric emptying GLP-1 is secreted from the L-cells in the intestine • Reduces food intake • Improves insulin sensitivity Long term effectsdemonstrated in animals… This in turn… • Increases beta-cell mass and maintains beta-cell efficiency Drucker DJ. Curr Pharm Des 2001; 7:1399-1412Drucker DJ. Mol Endocrinol 2003; 17:161-171
28-Day Exenatide Treatment in Type 2 Diabetes: Change in A1C at Day 28 Placebo Exenatide BID (bd) Exenatide BID (bhs) Exenatide TID (bds) 0 Baseline -0.2 (BYETTA) -0.4 Mean (SE)Change in A1C (%) -0.6 -0.8 * -1.0 * * -1.2 Intent to treat population (N=109); * P <0.006 BID (bd) = breakfast, dinner; BID (bs) = breakfast and bedtime; TID (bds) = breakfast, dinner, bedtime. Data from: Fineman MS, et al. Diabetes Care 2003; 26:2370-2377
Improvement in Cardiovascular Risk Factors with 3.5 Years of Exenatide Treatment (n = 151)Change from Baseline LDL-C (mg/dL) -11.8 ± 2.9 0.0001 Systolic Blood Pressure (mmHg) -3.5 ± 1.2 -2% 0.0001 Diastolic Blood Pressure (mmHg) -3.3 ± 0.8 -4% HDL-C (mg/dL) 8.5 ± 0.6 +24% 0.0001 Triglycerides (mg/dL) -44.4 ± 12.1 -12% 0.0003 Total Cholesterol (mg/dL) -10.8 ± 3.1 -5% 0.0007 Weight loss avg 5.3 kg Klonoff DC, et al. Curr Med Res Opin 2008;24:275-286 Nausea main side effect (use 20 minutes before meals), pancreatitis possible. Do not use Cr Cl <30 Caution CrCl <50
Liraglutide (Victoza) • 0.6 mg / day starting dose • Titrate 1.2-1.8 mg / day Multidose pens • Reduces postmeal glucose (A1c – 1% lower) • Nausea most common side effect • Associated with pancreatitis in rare instances • Use with metformin, sulfonylureas, TZD • Weight loss 2 kg/26 weeks • Medullary carcinoma in animals
meal Intestinal GLP-1 release T1/2 = 1 to 2 min Active GLP-1 DPP-4 GLP-1 inactive (>80% of pool) GLP-1 Secretion and Inactivation DPP-4 = dipeptidyl peptidase 4; GLP-1 = glucagon-like peptide–1.Deacon CF, et al. Diabetes. 1995;44:1126-1131.
0 0 –10 –10 –20 –20 –30 –30 –40 –40 –50 –50 –60 –60 Sitagliptin Monotherapy (Januvia) Significantly Lowers FPG and PPG Levels 24-week placebo-adjusted results FPG 2-Hour PPG Mean Baseline: 170 mg/dL Mean Baseline: 257 mg/dL P<0.001* P<0.001* n = 201 n = 234 –17† Mean Change in 2-Hour PPG, mg/dL‡ Mean Change in FPG, mg/dL‡ (95% CI: –24, –10) –47† (95% CI: –59, –34) *Compared with placebo. †Least-squares means adjusted for prior antihyperglycemic therapy status and baseline value. ‡Difference from placebo. CI=confidence interval; FPG=fasting plasma glucose; PPG=postprandial plasma glucose (meal challenge test). Aschner P et al. Diabetes Care. 2006;29:2632–2637.
Sitagliptin: Once-Daily Dosing—Proven 24-Hour Glycemic Control Patients With Renal Insufficiency*,† A dosage adjustment is recommended in patients with moderate or severe renal insufficiency and in patients with end-stage renal disease requiring hemodialysis or peritoneal dialysis. Assessment of renal function is recommended prior to initiation and periodically thereafter. * can be taken with or without food. †Patients with mild renal insufficiency—100 mg once daily. ‡ESRD=end-stage renal disease requiring hemodialysis or peritoneal dialysis.
Saxagliptin (Onglyza) • 2.5, 5 mg • Lowers A1c about 0.5-1% • May be used with dose adjustment in renal insufficiency • No weight loss
Bile Acid Binding ResinColesevelam (Welchol) • Approved for use in Type 2 diabetes • Lowers A1c by 0.8% 625 mg x 6/day • Add on to metformin • May increase triglycerides when used with sulfonylurea or insulin. • Don’t use when triglycerides are >500 • Many have GI side effects • May cause malabsorption of medications
New 2009 AACE/ACE Algorithm Lifestyle Modification A1c 6.5–7.5%* A1c 7.6–9.0% A1c > 9.0% Monotherapy Drug Naive Under Treatment Dual Therapy8 Symptoms No Symptoms 2–3 months† INSULIN ± Other Agent(s)6 INSULIN ± Other Agent(s)6 Dual Therapy 2–3 months† Triple Therapy9 2–3 months† Triple Therapy 2–3 months† INSULIN ± Other Agent(s)6 2–3 months† INSULIN ± Other Agent(s)6 Rodbard HW, et al . Endocrine Practice. 2009;15(6):540-559.
Action Profiles of Insulins Aspart, glulisine, lispro 4–5 hours Regular 6–8 hours NPH 12–16 hours Detemir ~14 hours Plasma Insulin Levels Glargine ~24 hours 0 2 3 4 5 6 7 8 9 12 13 14 15 16 17 18 19 20 21 22 23 24 1 10 11 Hours Burge MR, Schade DS. Endocrinol Metab Clin North Am. 1997;26:575-598; Barlocco D. Curr Opin Invest Drugs. 2003;4:1240-1244; Danne T et al. Diabetes Care. 2003;26:3087-3092
CASE 1 • 43 year Type 2 diabetes for 10 years • Admitted for CABG • Smoker 2 PPD, BP 160/90 • 100 KG HbA1c 9.9% • 20 mg glyburide • 2000 mg metformin • AM 2h noon 2h dinner 2h hs • 250 340 270 360 260 320 240 • What to do?
Case 1 what to do • Basal Insulin 0.5-2 units/kg/day • Bolus insulin = MS + Correction factor • Stop metformin Stop glyburide
Case 1 • Going home • What to do about control of diabetes • Basal/ bolus insulin therapy +/- metformin • Teach patient to adjust • Stop smoking! Needs 2 BP meds • Decrease CHO intake. 6 starches/day
Implementing New Titration Strategies With a Basal Insulin • An ADA/EASD consensus algorithm for the initiation and adjustment of a basal insulin regimen at 10 IU per day is indicated as follows: Start with a long-acting basal insulin, initiated at 10 IU/day Check fasting glucose daily and increase dose by 2 IU every 3 days until fasting levels are in target range (70-130 mg/dL) ADA, American Diabetes Association; EASD, European Association for the Study of Diabetes. Please see Important Safety Information for LANTUS® on slides 38-39. Please see accompanying full Prescribing Information for LANTUS®. Nathan et al. Diabetes Care. 2006;29:1963-1972.
Case 3 • 20 yo female with type 1 diabetes for 8 years comes to the hospital for elective surgery. Weight 50 kg • Does not check her blood glucose and takes 70/30 insulin 40 units in the AM and has hypoglycemia daily at 11 AM • What to do?
Case 3 • All patients with Type 1 diabetes should be on basal bolus insulin therapy. 70/30 insulin is usually not useful and once per day does not provide adequate coverage. • Type 1 requires 24 hour coverage • Obtain A1c 14% • Total dose 0.5-1 unit/kg/day • ½ basal ½ bolus
Action Profiles of Insulins Detemir ~14 hours Plasma Insulin Levels Glargine ~24 hours 0 2 3 4 5 6 7 8 9 12 13 14 15 16 17 18 19 20 21 22 23 24 1 10 11 Hours Burge MR, Schade DS. Endocrinol Metab Clin North Am. 1997;26:575-598; Barlocco D. Curr Opin Invest Drugs. 2003;4:1240-1244; Danne T et al. Diabetes Care. 2003;26:3087-3092
What does basal insulin cover? • Excessive gluconeogenesis • Does this occur in the hospital? • Does stress occur in the hospital? • Protein and fat intake to some extent
Action Profiles of Insulins Aspart, glulisine, lispro 4–5 hours Regular 6–8 hours Plasma Insulin Levels 0 2 3 4 5 6 7 8 9 12 13 14 15 16 17 18 19 20 21 22 23 24 1 10 11 Hours Burge MR, Schade DS. Endocrinol Metab Clin North Am. 1997;26:575-598; Barlocco D. Curr Opin Invest Drugs. 2003;4:1240-1244; Danne T et al. Diabetes Care. 2003;26:3087-3092
Bolus insulin • Meal supplement Mainly covers carbohydrate • Helps with protein and fat coverage • Correction factor • Compensates for insufficient basal insulin or insufficient meal supplement • If NPO use regular insulin q 6 hours
BOLUS COVERAGE • Correction factor • May use anytime • Meal times are convenient • x units/ y mg%> z mg% • Insulin resistance • Type 2 2 – 4 units/50 mg%>150 mg% • Type 1 1- 2 units/50mg% >150 mg%
BOLUS INSULIN- GO FIGURE: • Meal coverage • Counting carbohydrates • 1 unit / 5-10 gm CHO Type 2 • 1 unit/ 10-15 gm CHO Type 2 • Can’t count carbs? MD count them and estimate the meal supplement
Insulin Injection Devices Insulin Pens • Faster and easier than syringes • Improve patient attitude and adherence • Have accurate dosing mechanisms, but inadequate resuspension of NPH may be a problem
Case of the uncontrollable glucose admitted infection • 52 year Type 2 diabetes • 200 kg HbA1c 9.9% • Stage 2 renal disease • 20 mg glyburide, precose 50mg ac • 2000 mg metformin, januvia 100mg/day • 125 units of Glargine BID • AM 2h noon 2h dinner 2h hs • 340 440 320 450 320 510 450