Download

1 / 49
500 likes | 710 Views
Financing Health Care. Why is this an ethical concern?. “The United States has the best health care system in the world.”. “In short, the health care system in the United States is an embarrassing, world-class mess.”. -- Davidoff and Reinecke, editorial, Annals of Internal Medicine, 1999.

E N D
Financing Health Care Why is this an ethical concern?
“The United States has the best health care system in the world.”
“In short, the health care system in the United States is an embarrassing, world-class mess.” -- Davidoff and Reinecke, editorial, Annals of Internal Medicine, 1999
Why the difference? • Is it just a matter of the technological capacity of the health care system, for patients who enjoy full access? • Or is it also a matter of the ethics and fairness of access and the distribution of resources?
Financing Health Care • Economic • Political • Legal • Public policy • Ethical?
Is Health Care Special? • Is health care a market commodity-- • Like a VCR? • Is health care a special social good-- • Like basic education? • Is health care a right-- • Like right to vote and right to a jury trial?
Health Care as Right • Wide variation in how much various people “need” through life • With rapid advances in technology, what is “basic minimum” of care keeps changing • Seems more clear and persuasive to see health care as important social good, not right
Market Commodity? • Reinhardt: Child of a poor US family with a chronic but treatable disease may have much more serious interference of health with basic life chances than richer child with same disease
Market Commodity?-- II • Is this unfortunate? • Like a hurricane • Is this unfair? • Like racial profiling
Libertarian position • Unfortunate but not unfair • If poor could simply demand health care they cannot afford, they would be stealing goods from others who have worked hard to accumulate them • Rich may voluntarily create private charities to help poor
Against Libertarianism • Are health care knowledge and skills purely the result of one’s private labor and effort, or has society at large heavily subsidized the training and research process at each step? • (E.g., estimated that a medical student pays 5% of the total cost of education)
Leonard Fleck’s argument on the basically unfair nature of today’s health care system in the U.S.
Fast Food Worker • Near minimum wage • Pays taxes • No health benefits • Not eligible for Medicaid • Example of working poor who are most of uninsured in US
MSU Professor • Fairly well paid • Receives health insurance as benefit • Benefits are not taxed • Therefore other taxpayers subsidize health insurance
Health Insurer • Spends a lot to assure that benefits are not paid to any uncovered members • Adds to high administrative cost of US health care (enough extra to pay for all care for uninsured)
Two Myths • The uninsured generally wish to be uninsured and do not suffer any ill health • We’d have plenty of money for all the health care anyone could want if not for waste, fraud and abuse
Uninsured in U.S. • Less likely to see doctor • More likely to delay hospital care • Less likely to get preventive care • Chances of dying in hospital 24% to 124% greater depending on age and income
Question • What would it cost to provide the highest possible standard of medical care for every person in the U.S.?
Answer • Nine times the GDP
Savings from Waste/Fraud Slope of curve based on new technology, aging Costs once again rising Eliminate all waste, fraud
Another Myth • Universal coverage may be an ethically nice idea, but it would cost way too much to be economically feasible
Conclusions in Two State Commissions • If state could adopt a single-payer model with universal coverage, savings would be enough to pay for the care of all the currently uninsured • Michigan • Maryland
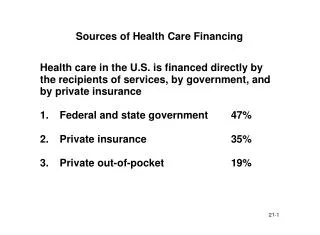
Why Excess Administration? • Multiple payers -> great duplication of services • Each payer has to hire staff to assure that it does not pay for anyone else’s enrollees • Typical administrative overhead • US private insurance company 15-20% • Medicaid, Medicare 3-5%
A Quiz • Canada has national health insurance, so essentially everything spent on health care is public $$ • US supposedly has a largely “free market” system, but we have some government programs • How does per personpublic spending compare in US and Canada?
Health Expenditures in Public Funds Only per capita, 1994 US figures do NOT include tax subsidies for employer-paid health insurance
Congressional Budget Office 1994 • Two health plans then being proposed before Congress led to cost savings in 10 years and after • BOTH plans proposed universal coverage • None of various other plans saved money • None of the other plans proposed universal coverage • Same is true internationally
Why Not the Marketplace? • No one has so far proposed a genuinely “free-market” answer to the problem of universal coverage • In addition, the marketplace “solutions” that seem most popular today have their own major problems
The Insurance Ideal (e.g. Fire) • Financial protection against low-probability but catastrophic event • Affordable and practical because all who are at risk pay into the pool • Most of the cost for those who receive benefits come out of the pockets of those who never suffer the harm
Health “Insurance”? • Virtually everyone gets some health care sooner or later-- most get some each year • Strong incentives for those at low risk to avoid paying for those at high risk • “Risk adjustment” potentially huge (vs. smoke alarms)
Disproportionate Costs • Light: • 5% of population use half of resources • 10% of population use 70% of resources • Therefore huge competitive advantage to insurer if it can exclude a relatively small subset of patients from coverage • “Inverse coverage law” (Light)-- systematic discrimination against neediest people
“Medically Uninsurable” • Example: You work in a small business with 7 other people • Employer provides a group policy • One of the other 7 workers develops multiple sclerosis • Insurer cancels plan or triples premium • You lose
Case Study: Medicare HMO’s • Managed care had history of providing good quality care at lower cost • More efficient • Competition was excessively wasteful • “Cherry picking” (selective marketing) • Therefore, could save huge sums by converting Medicare to HMO plans
Medicare HMO’s (cont.) • Created incentives for private insurers to contract to provide HMO care for Medicare beneficiaries • Agreed to pay capitation rates of about 90% of current per-person Medicare costs (assuming this would be stimulus for efficiency) • Insisted on free choice
Medicare HMO’s (cont.) • Insurers turned out to be very good at marketing plans to the healthiest seniors whose true cost of care was only 60-80% of average • In “free choice” system, the sickest elderly remained in the non-HMO pool, essentially having U.S. taxpayer underwrite the profits of the HMOs
Medicare HMO’s (cont.) • After 2-3 years and tighter control: • Either seniors complained of poor services and disenrolled from HMOs; or • Insurers decided to make desired profits they had to greatly increase premiums • Result: Most Medicare HMOs went out of business, after insurer had collected windfall profits at expense of U.S. taxpayer
Medical Savings Accounts • Heavily supported by insurance lobbyists (as were Medicare HMOs) • Ideal: let law of supply and demand operate in a system that previous has been relatively immune • Combine MSA with high-deductible catastrophic health insurance
Medical Savings Accounts- II • Example: $3000-deductible insurance and $3000 in MSA • Because you get to keep what’s left in MSA at end of year, you are going to be a “smart shopper” of health care • For doctors: less paperwork since a lot of care is cash-reimbursed
Problems with MSAs • If you know that your yearly care is going to exceed MSA limit, lose all incentive for “shopping” • “Anti-insurance”-- if you get to take money out of pool because you are low risk, no money remains in pool to pay for those at high risk
Problems with MSAs • Predict that healthiest will buy MSAs and sickest will not (adverse selection) • Therefore “public safety net” will pay for the care of the sick while the healthy make personal profits on their MSAs (again: taxpayers subsidize the profits of the healthy and the insurance companies)
Problems with MSAs-- III • International example: Singapore • After a 10 year trial, had to scratch plan because health care costs rose out of control
Problems with MSAs-- IV • Light: Not to be your brother’s keeper is actuarially sound but ethically unsound • But it also drives up costs for all because administrative costs are higher to extent that insurers have incentives to use selective marketing, risk rating, etc.
Conclusion • A patchwork of multiple payers with no guarantee of universal coverage is: • Ethically unacceptable in a well-off society • Economically inefficient • Various aspects of competitive marketplace may be combined with universal coverage (e.g., Germany)
Ethics and the Clinton Plan • Why worth studying? • While plan was a political failure it was only recent effort to assure universal coverage • Political failure was arguably due to reasons unrelated to ethics of plan • Ethics could have guided an open-ended inquiry for a better plan had political will existed
Major Ethical Conflict • “Individual choice and responsibility” value cluster • “Community solidarity” value cluster • USA is the only advanced country where the example of the person who irresponsibly ruins his/her own health has successfully derailed a centralized health plan for all
The American people can be counted on to do the right thing, after they have exhausted all other possibilities. --Winston Churchill