Download
1 / 22
230 likes | 621 Views
Newer Psychotropic Drugs. Guy Brookes Leeds PFT. Content. Antipsychotic Medication Antidepressant Medication Mood Stabilisers What does the Evidence mean?. Antipsychotic Medication. The baseline Symptom clusters – Positive, Negative (1⁰, 2⁰), Affect, Cognitive, Disorganised

E N D
Newer Psychotropic Drugs Guy Brookes Leeds PFT
Content • Antipsychotic Medication • Antidepressant Medication • Mood Stabilisers • What does the Evidence mean?
Antipsychotic Medication • The baseline • Symptom clusters – Positive, Negative (1⁰, 2⁰), Affect, Cognitive, Disorganised • Efficacy – No difference for positive symptoms • Effectiveness and Limitations • Action of antipsychotics • Dopamine (D2)- Pathways
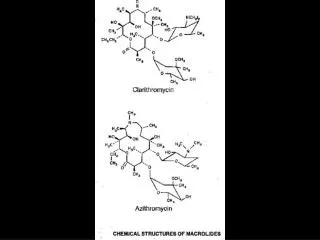
Newer Antipsychotics • Atypical antipsychotics • Serotonin / Dopamine antagonists • Risperidone • Olanzapine • Amisulpiride • Quetiapine • Aripiprazole
Clozapine • Prototype for Atypicals • Only Antipsychotic with greater efficacy for Positive symptoms and good evidence for Negative symptoms • Neutropenia • Sedation, Weight gain, Hypersalivation, Fits • Specific indications • NICE Guidance
Risperidone • “Atypical” at lower doses • Key side effects • EPSE, Prolactin (relative) • Sexual side effects • Start 2mg increase to c.4/6mg (max. 16mg) • Single night dose • Less weight gain • Not if risk of stroke • Velotabs, Depot, • Not if risk of stroke
Olanzapine • Very similar to Clozapine • Key side effects • Weight gain • Sedation • Start 10mg. Up to 20mg. • Single night dose • Safe • Low incidence: EPSE, 2⁰Neg, ↑Prolactin, • Velotabs and IM • Not if risk of stroke • Mood stabiliser, Treatment Resistant depression, Anxiety
Quetiapine • Similar to Clozapine • Dose: Titrate from 25mg to c. 600mg (max 750mg) • Very low EPSE or Prolactin change • Some sedation – problematic as bd dosing • Less weight gain than other atypicals • Titration over several days • Less effective at low/mid doses • For schizophrenia need 600mg per day • Also for BPAD
Amisulpiride • Not really atypical. Little serotonergic effect • Sedation generally low • Negative symptoms at low dose • Key side effects • EPSE, Raised Prolactin • Little weight gain • Dose 200mg bd to 400mg bd (max 1200mg)
Aripiprazole • Partial Agonist – NB Frontal lobe • Newest • Little sedation, EPSE, weight gain • Key side effects • Agitation • Nausea • Theoretically effective for Negative symptoms • Start 10mg od. Up to 30mg • People’s favourite?
Antidepressants • Baseline • Depressive illness v’s unhappiness • Effect size – severity, trial, placebo • Practical difficulties • Comparator bias • Action • Serotonin / Noradrenalin / both
New Antidepressants • SSRIs – latest developments • Mirtazepine • Duloxetine • Escitalopram
The trouble with….SSRIs • Effectiveness and Efficacy • Depressive illness – definition • Mild depression / adjustment • Efficacy increases with severity and duration of trial • Publication bias, Placebo increasing with time. • Study design – ITT, Rating scale, duration, age • Suicidality • Agitation / Akathisia • Anxiety, Sexual dysfunction…….. • Overuse / social changes
Mirtazepine • Dual acting • NICE – no greater efficacy • Start 30mg (15mg). Up to 45mg • Key side effects • Sedation (greater at low dose) • Weight gain • Generally well tolerated, safe. • Also for anxiety disorders
Duloxetine • Dual acting • Dose 30 – 60mg. Single dose • Key side effects • GI symptoms, anxiety, agitation • Stress incontinence • No evident greater effcicacy
Escitalopram • Theoretically should produce fewer side effects – Serotonergic. • Generally no fewer drop-outs in studies. • No clear clinical benefit over SSRIs • Start 10mg – can increase though evidence unclear (max. 20mg)
Outcome • Efficacy • Antidepressants no more effective than placebo for mild depression. • Primary care – no difference • Secondary care – Venlafaxine, ?Escitalopram > SSRI • Inpatient – TCA > SSRI • SSRIs more likely to be prescribed at therapeutic dose for therapeutic period • Structured interventions around prescribing more effctive • Side effects • Newer antidepressants may be better tolerated than TCAs • Different • Concordance
Mood Stabilisers • Effects • Prophylactic, Mania, Depression • Anti-epileptic • Valproate, CBZ, Lamotrigine, Gabapentin, Topiramate • Lithium • Antipsychotic • Olanzapine, Quetiapine, Aripiprazole
Lamotrigine • Probably prevents depressive more than manic episodes • Generally up to 200mg day • Slow titration upwards – Stevens Johnson Synd. • NICE – not first line treatment
Depakote • Licensed for Mania
Other Mood Stabilisers • Gabapentin • No efficacy in BP Depression • Inferior to Placebo in Mania • Not recommended by NICE • Topiramate • No evidence of efficacy • Not recommended by NICE • Antipsychotics • Olanzapine, Quetiapine, Aripiprazole