Download
1 / 1
10 likes | 253 Views
Leadership is one of six health system building blocks 1.2 Leadership influences the function and effectiveness of other building blocks 1 Effective leadership is a key feature of successful health systems 1,2,3

E N D
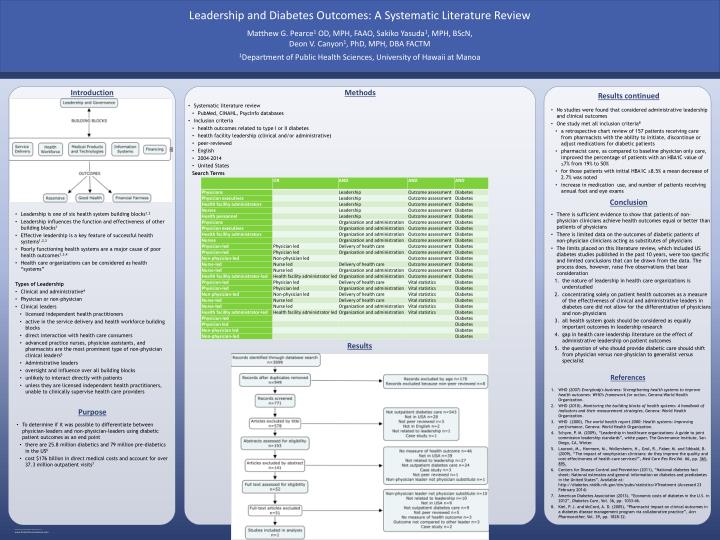
Leadership is one of six health system building blocks1.2 Leadership influences the function and effectiveness of other building blocks1 Effective leadership is a key feature of successful health systems1,2,3 Poorly functioning health systems are a major cause of poor health outcomes1,3,4 Health care organizations can be considered as health “systems” Types of Leadership Clinical and administrative4 Physician or non-physician Clinical leaders • licensed independent health practitioners • active in the service delivery and health workforce building blocks • direct interaction with health care consumers • advanced practice nurses, physician assistants, and pharmacists are the most prominent type of non-physician clinical leaders5 • Administrative leaders • oversight and influence over all building blocks • unlikely to interact directly with patients • unless they are licensed independent health practitioners, unable to clinically supervise health care providers Introduction Purpose Systematic literature review PubMed, CINAHL, PsycInfo databases Inclusion criteria health outcomes related to type I or II diabetes health facility leadership (clinical and/or administrative) peer-reviewed English 2004-2014 United States Search Terms Methods Results continued There is sufficient evidence to show that patients of non-physician clinicians achieve health outcomes equal or better than patients of physicians There is limited data on the outcomes of diabetic patients of non-physician clinicians acting as substitutes of physicians The limits placed on this literature review, which included US diabetes studies published in the past 10 years, were too specific and limited conclusions that can be drawn from the data. The process does, however, raise five observations that bear consideration the nature of leadership in health care organizations is understudied concentrating solely on patient health outcomes as a measure of the effectiveness of clinical and administrative leaders in diabetes care did not allow for the differentiation of physicians and non-physicians all health system goals should be considered as equally important outcomes in leadership research gap in health care leadership literature on the effect of administrative leadership on patient outcomes the question of who should provide diabetic care should shift from physician versus non-physician to generalist versus specialist References To determine if it was possible to differentiate between physician-leaders and non-physician-leaders using diabetic patient outcomes as an end point there are 25.8 million diabetics and 79 million pre-diabetics in the US6 cost $176 billion in direct medical costs and account for over 37.3 million outpatient visits7 Matthew G. Pearce1 OD, MPH, FAAO, Sakiko Yasuda1, MPH, BScN, Deon V. Canyon1, PhD, MPH, DBA FACTM 1Department of Public Health Sciences, University of Hawaii at Manoa Leadership and Diabetes Outcomes: A Systematic Literature Review WHO (2007) Everybody's business: Strengthening health systems to improve health outcomes: WHO's framework for action,Geneva:World Health Organization. WHO (2010), Monitoring the building blocks of health systems: A handbook of indicators and their measurement strategies, Geneva: World Health Organization. WHO (2000), The world health report 2000: Health systems: Improving perfromance, Geneva: World Health Organization. Schyve, P. M. (2009), “Leadership in healthcare organizations: A guide to joint commission leadership standards”, white paper, The Governance Institute, San Diego, CA, Winter. Laurant, M., Harmsen, M., Wollersheim, H., Grol, R., Faber, M. and Sibbald, B. (2009), “The impact of nonphysician clinicians: do they improve the quality and cost-effectiveness of health care services?”, Med Care Res Rev,Vol. 66, pp. 36S-89S. Centers for Disease Control and Prevention (2011), “National diabetes fact sheet: National estimates and general information on diabetes and prediabetes in the United States”, Available at: http://diabetes.niddk.nih.gov/dm/pubs/statistics/#Treatment (Accessed 23 February 2014) American Diabetes Association (2013), “Economic costs of diabetes in the U.S. in 2012”, Diabetes Care, Vol. 36, pp. 1033-46. Kiel, P. J. and McCord, A. D. (2005), “Pharmacist impact on clinical outcomes in a diabetes disease management program via collaborative practice”, Ann Pharmacother, Vol. 39, pp. 1828-32. No studies were found that considered administrative leadership and clinical outcomes One study met all inclusion criteria8 a retrospective chart review of 157 patients receiving care from pharmacists with the ability to initiate, discontinue or adjust medications for diabetic patients pharmacist care, as compared to baseline physician only care, improved the percentage of patients with an HBA1C value of ≤7% from 19% to 50% for those patients with initial HBA1C ≥8.5% a mean decrease of 2.7% was noted increase in medication use, and number of patients receiving annual foot and eye exams Conclusion Results