Download
1 / 39
410 likes | 475 Views
Discover the key statistics, risk factors, and prevention methods associated with ACL injuries. From the cost of reconstruction to the failure rates, learn about the modifiable and non-modifiable risk factors and the impact of neuromuscular imbalances. Explore how hormone function, ligamentous laxity, and environmental factors play a role in ACL injury prevention. Find out about the importance of balance, strength, proprioception, and more in effective ACL injury prevention programs.

E N D
ACL Injury Prevention Programs Michael D. Lee, MD
ACL Tears • 250,000 to 300,000 per year • $20,000 to $50,000 per reconstruction • $800 to $3000 out of pocket • PT: $1000+
ACL Reconstruction Failure Rate • 6% ipsilateral knee (2-10%) • 12% contralateral knee (8-16%) • about 1 in 5 will have another ACL tear Wright et al., JBJS, 2011
ACL Revision Failure Rate • 14% Wright et al., JBJS, 2012
ACL Tears • ACL reconstructed knee is not “normal” • lifelong increased risk of OA • best treatment: prevention
Female Risk • 4 - 6 times male risk • Title IX 1972 Act • Female participation 5 times at college level • Female participation 10 times high school level
ACL Injuries • 70% are non-contact injuries • Non-contact injuries are theoretically preventable
Risk Factors • non-modifiable • modifiable basis for prevention
Non-modifiable Risk Factors • anatomic • genetic: COL5 risk in some females • developmental • hormonal • Ge • G
Notch Stenosis • Theory: small notch impinges on ACL • Several studies support this theory
Notch Size • Smaller notch = smaller ACL? • + correlation of ACL size and notch width index • Smaller ACL found in ACL injured patients compared to controls
Ligamentous Laxity • Generalized LL a significant risk for ACLI • Studies show knee hyperextension in ♀ soccer and bball players a risk for ACLI
Tibial Slope • Increased slope increases ACLI risk • Increased slope increases ACL strain
Hormonal Function • ACL fibroblasts have estrogen receptors • Estrogen affects tensile properties of ligaments • Increased ACLI risk in pre-ovulatory menstrual phase (first 1/2 of cycle)
Hormone Function • Retrospective studies show decreased risk of ACLIs with BCPs • Theory: stabilize hormonal functional through cycle
Neuromuscular Maturation • No ACLI difference in pre-adolescent ♀vs ♂ • 4 -6 x risk for females after maturation • only males have a n-m spurt with increase in power, strength and coordination • post-maturation jump mechanics differ
Modifiable Risk Factors Neuromuscular Imbalance • ligament dominance • quadriceps dominance • leg dominance • trunk dominance
Ligament Dominance • responsible for valgus collapse • supporting ms groups don’t adequately contract to absorb ground reaction forces • this increases the forces placed thru static restraints
Ligament Dominance • all LE muscles contribute to dynamic stability • posterior kinetic chain most important for ACLI prevention (glutes, hamstrings, gastro-soleus) • improper PKC recruitment during landing causes higher knee abd. moments and increases load on ACL
Quadriceps Dominance • ♀ preferentially activate quads in landing • results in stiff-legged, extended landing posture rather than safer flexed position • hamstrings are ACL-agonists, reducing anterior tibial translation • Quads are ACL-antagonists, exerting strain on ACL
Quadriceps Dominance • an erect or extended knee landing posture activates the quads • quadriceps contraction increase anterior shear stress to knee • protective pull of hamstrings is lost • plyometric training can increase HS:Quad torque or strength ratio
Leg Dominance • women rely more on one leg compared to men • leg dominance defined as measurable muscle asymmetry • limited evidence to support LD as a definite risk factor
Trunk Dominance • inability to control trunk in space allows greater movements outside of safe zone • creates larger moments on the LE • ACL injured females in one study had significantly more max. trunk displacement in all directions compared to controls
Environmental • most important is shoe-surface interface • larger (longer) cleats and rubber floors are risk factors in several studies
Fatigue • may decrease dynamic stability • Chappell et al: increased ant shear force and valgus moments, and decreased flexion angles in jump study in fatigued vs non-fatigued state • data support but clinical research lacking to validate this theory
Prevention Focus • balance • strength • proprioception • endurance • plyometrics • stability
Goals Prevention Biomechanics • decrease peak landing forces, knee abduction forces and HS/Quad strength ratio • increase knee flexion with landing • importance of feedback can’t be overemphasized
Clinical Studies • Hewett et al. 1999, 1263 athletes: increased ACLI in untrained group • Mandelbaum “PEP” program: Prevent injury and Enhance Performance. 20 min. soccer program replaces warm-up. Reduced ACLI 74-88% over 2 years
Clinical Studies • Gilchrist et al.: 1435 female Div. I soccer players. Non-contact ACLI rate 3.3 x less in trained group • Caraffa et al.: Proprioceptive training 600 soccer players. ACLI 8 x higher in untrained group
Meta-Analyses of ACL PP • Hewett 2006: 6 studies, concluded that N-M programs have sign. effect on reducing ACLIs • Yoo 2010: ACLI PP best for < 18 y.o., female, and emphasis on plyometric and strength training. • Sadoghi 2012: significant, positive effect of ACLI PP. ♀ RRI = 52%. ♂ RRI = 85%
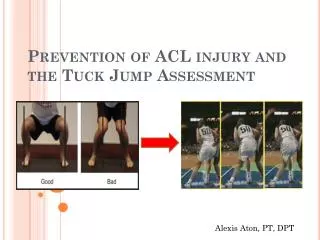
Screening • Meyer: ♀ separated into hi/low risk groups from motor analysis of drop vertical jump. Significant decrease in knee abduction moments in hi risk group with ACLI PP training. • DiStefano: “LESS”: Landing Error Scoring System. Those with higher risk scores improved most with ACLI PP
Screening • Studies consistently identify at risk athletes • identification methods presently are too labor intensive for large scale implementation.
Compliance • Poor • athletes and coaches prefer to focus on performance rather than injury prevention
Compliance • Performance is usually enhanced with ACLI PP • Improved: LE strength, vertical jump height, • squat strength, single leg hop distance, sprint times
Recommendations Journal of Bone and Joint Surgery 2013 • “ all female athletes should undergo an ACL PP until more reliable methods of identification of at-risk athletes are developed. The training sessions should emphasize proper technique and should be performed year-round.”