Download
1 / 1
10 likes | 185 Views
ASSESSMENT AND REVIEW OF HIV POSITIVE PATIENT MEDICAL RECORDS FROM A TRADITIONAL SIDDHA MEDICINE HOSPITAL IN TAMIL NADU, INDIA . Scott Ikeda, Kaylan Baban, Deeangelee Pooran, Nils Hennig MD/PhD, George Carter, Debbie Indyk PhD, Henry Sacks MD/PhD,

E N D
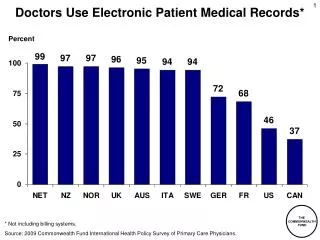
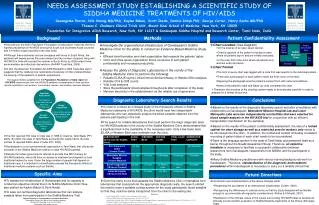
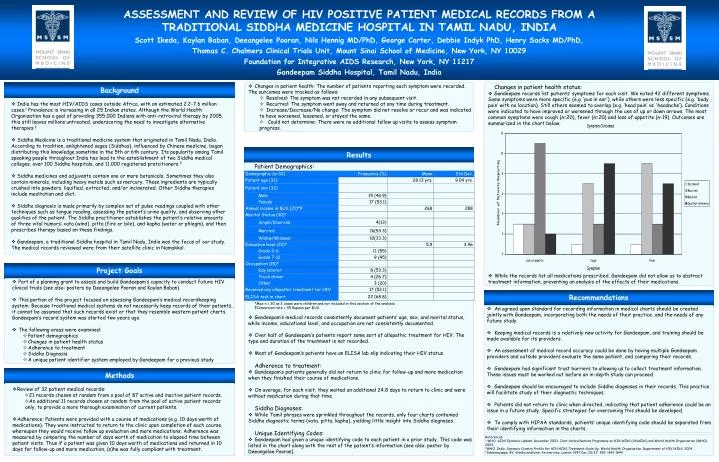
ASSESSMENT AND REVIEW OF HIV POSITIVE PATIENT MEDICAL RECORDS FROM A TRADITIONAL SIDDHA MEDICINE HOSPITAL IN TAMIL NADU, INDIA Scott Ikeda, Kaylan Baban, Deeangelee Pooran, Nils Hennig MD/PhD, George Carter, Debbie Indyk PhD, Henry Sacks MD/PhD, Thomas C. Chalmers Clinical Trials Unit, Mount Sinai School of Medicine, New York, NY 10029 Foundation for Integrative AIDS Research, New York, NY 11217 Gandeepam Siddha Hospital, Tamil Nadu, India Background • Changes in patient health: The number of patients reporting each symptom were recorded. The outcomes were tracked as follows: • Resolved: The symptom was not recorded in any subsequent visit. • Recurred: The symptom went away and returned at any time during treatment. • Increase/Decrease/No change: The symptom did not resolve or recur and was indicated to have worsened, lessened, or stayed the same. • Could not determine: There were no additional follow up visits to assess symptom progress. Changes in patient health status: • Gandeepam records list patients’ symptoms for each visit. We noted 42 different symptoms. Some symptoms were more specific (e.g. ‘pus in ear’), while others were less specific (e.g. ‘body pain’ with no location). Still others seemed to overlap (e.g. ‘head pain’ vs. ‘headache’). Conditions were indicated to have improved or worsened through the use of up or down arrows. The most common symptoms were cough (n=20), fever (n=20) and loss of appetite (n-19). Outcomes are summarized in the chart below: • While the records list all medications prescribed, Gandeepam did not allow us to abstract treatment information, preventing an analysis of the effects of their medications. India has the most HIV/AIDS cases outside Africa, with an estimated 2.2-7.6 million cases.1 Prevalence is increasing in all 25 Indian states. Although the World Health Organization has a goal of providing 355,000 Indians with anti-retroviral therapy by 2005, this still leaves millions untreated, underscoring the need to investigate alternative therapies.2 Siddha Medicine is a traditional medicine system that originated in Tamil Nadu, India. According to tradition, enlightened sages (Siddhas), influenced by Chinese medicine, began distributing this knowledge sometime in the 5th or 6th century. Its popularity among Tamil speaking people throughout India has lead to the establishment of two Siddha medical colleges, over 100 Siddha hospitals, and 11,000 registered pratcitioners.3 Siddha medicines and adjuvants contain one or more botanicals. Sometimes they also contain minerals, including heavy metals such as mercury. These ingredients are typically crushed into powders, liquified, extracted, and/or incinerated. Other Siddha therapies include meditation and diet. Siddha diagnosis is made primarily by complex set of pulse readingscoupled with other techniques such as tongue reading, assessing the patient’s urine quality, and observing other qualities of the patient. The Siddha practitioner establishes the patient’s relative amounts of three vital humors: vata (wind), pitta (fire or bile), and kapha (water or phlegm), and then prescribes therapy based on these findings. Gandeepam, a traditional Siddha hospital in Tamil Nadu, India was the focus of our study. The medical records reviewed were from their satellite clinic in Namakkal. Results Patient Demographics: Project Goals • Part of a planning grant to assess and build Gandeepam’s capacity to conduct future HIV clinical trials (see also: posters by Deeangelee Pooran and Kaylan Baban). • This portion of the project focused on assessing Gandeepam’s medical recordkeeping system. Because traditional medical systems do not necessarily keep records of their patients, it cannot be assumed that such records exist or that they resemble western patient charts. Gandeepam’s record system was started two years ago. • The following areas were examined: • Patient demographics • Changes in patient health status • Adherence to treatment • Siddha Diagnosis • A unique patient identifier system employed by Gandeepam for a previous study Recommendations *Max n = 30 as 2 cases were children and not included in this section of the analysis. ‡Conversion rate = 45 Rupees per $US. • Gandeepam’s medical records consistently document patients’ age, sex, and marital status, while income, educational level, and occupation are not consistently documented. • Over half of Gandeepam’s patients report some sort of allopathic treatment for HIV. The type and duration of the treatment is not recorded. • Most of Gandeepam’s patients have an ELISA lab slip indicating their HIV status. Adherence to treatment: • Gandeepam’s patients generally did not return to clinic for follow-up and more medication when they finished their course of medications. • On average, for each visit, they waited an additional 24.8 days to return to clinic and were without medication during that time. Siddha Diagnoses: • While Tamil phrases were sprinkled throughout the records, only four charts contained Siddha diagnostic terms (vata, pitta, kapha), yielding little insight into Siddha diagnoses. Unique Identifying Codes: • Gandeepam had given a unique identifying code to each patient in a prior study. This code was listed in the chart along with the rest of the patient’s information (see also: poster by Deeangelee Pooran). An agreed upon standard for recording information in medical charts should be created jointly with Gandeepam, incorporating both the needs of their practice, and the needs of any future study. Keeping medical records is a relatively new activity for Gandeepam, and training should be made available for its providers. An assessment of medical record accuracy could be done by having multiple Gandeepam providers and outside providers evaluate the same patient, and comparing their records. Gandeepam had significant trust barriers to allowing us to collect treatment information. These issues must be worked out before an in-depth study can proceed. Gandeepam should be encouraged to include Siddha diagnoses in their records. This practice will facilitate study of their diagnostic techniques. Patients did not return to clinic when directed, indicating that patient adherence could be an issue in a future study. Specific strategies for overcoming this should be developed. To comply with HIPAA standards, patients’ unique identifying code should be separated from their identifying information in the charts. Methods • Review of 32 patient medical records: • 21 records chosen at random from a pool of 87 active and inactive patient records. • An additional 11 records chosen at random from the pool of active patient records only, to provide a more thorough examination of current patients. • Adherence: Patients were provided with a course of medications (e.g. 10 days worth of medications). They were instructed to return to the clinic upon completion of each course, whereupon they would receive follow up evaluation and more medications. Adherence was measured by comparing the number of days worth of medication to elapsed time between patient visits. Thus if a patient was given 10 days worth of medications and returned in 10 days for follow-up and more medication, (s)he was fully compliant with treatment. References: 1 WHO. AIDS Epidemic Update: December 2003. Joint United Nations Programme on HIV/AIDS (UNAIDS) and World Health Organization (WHO). 2003. 2WHO. India, Summary Country Profile for HIV/AIDS Treatment Scale-Up. World Health Organization, Department of HIV/AIDS. 2004. 3Subbarayappa, BV. Siddha medicine: An overview. Lancet, 1997 Dec 20/27; 350: 1841-1844.