Download
1 / 22
230 likes | 317 Views
Learn how to identify and respond to signs of child abuse, neglect, and exploitation. Explore key indicators, case studies, and strategies for safeguarding children. Understand the risks, warning signs, and actions to take in cases of missing or at-risk children.

E N D
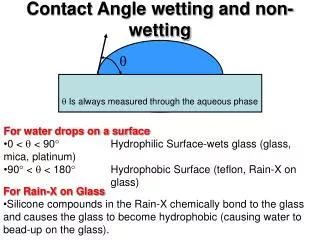
Wetting and Soiling Consider abuse if a child; Has secondary day or night wetting not responding to treatment Is reported to be deliberately wetting Shows encopresis (doing normal stools in the wrong place) or smearing
Case study A mother brings her 7 year-old daughter, Maya, about her eczema. You notice a 10cm x 6cm greenish bruise on the back of her thigh. Neither of them know how it got there. • What else do you want to know? • What will the outcome of the consultation be?
Suspicious bruises • Shape of a hand or objected or ligature • Petechiae with no cause • Immobile baby or child • Bruised face, eyes, ears, buttocks or non-boney area • Neck strangulation marks
Missing Children Children who go missing are extremely vulnerable to • Sexual exploitation and trafficking • Homelessness • Drug and alcohol abuse • Crime • Suicide • There are push and pull reasons for going missing
What to do about Missing Children The police and social care are the responsible agencies • Police 999 for urgent cases e.g. snatched child • Police 101 and the social care Missing Children Officer will liaise for less urgent cases • GP practices should consider referring all missing families to Social Care CAFD
Self Harm and Suicide CAMHS Crisis 0115 8440560 • Refer all under 18s expressing suicidal thoughts to CAMHS Crisis • Self harm is increasingly common • Always consider abuse as a reason or masquerading as self harm • It is still rare in primary school children and they should all be referred to Social Care
Child Sexual Abuse Child Sexual Exploitation (CSE): a type of sexual abuse in which children and young people are sexually exploited for money, power or status. • Asian gangs e.g. “3 Girls” TV docu-drama • Happens in all ethnic groups • Grooming can be fast or slow • Child may not realise, or be brutally assaulted
Q: When is a sexually active teenager a victim of abuse? A: When you don’t like their boyfriend • Too old (by more than 2y) • Too flash (gifts, phones, fast cars) • Too controlling (“gets you to do things you don’t want to”) • Multiple partners • Providing drugs/drink • 12y and under – statutory rape
How to talk to young people What does this doctor do well and less well? What is different this time? https://www.youtube.com/watch?v=B37oVxw8CZ4 7.33 • https://www.youtube.com/watch?v=B37oVxw8CZ4 • 2.36
Making an assessment GPs need to ask open questions and offer to see older children alone with a colleague, but mainly not spoil any evidence Explore in a non-leading way any presenting signs or history (but do not spoil evidence) Do not rely on only one person for information Include male and female parents and carers equally • Observe the child and interactions with parents • Communicate with the child without their parents present with the parent’s consent (GPs should only offer this to older children) • Acknowledge strengths and weaknesses of parenting
Risks for repeated and ongoing abuse Neglect and emotional abuse are more likely to persist and repeat than other forms of abuse Chronic parental stress Parent is survivor of child abuse or neglect • Parent non-engagement with services • Previous episodes of abuse or neglect • Mental health or substance abuse impacting on ability to parent
Why do clinicians miss abuse? • Concern about missing a treatable disorder/disease • Fear of alienating parents • Discomfort of thinking ill of parents or wrongly blaming them • Personal safety • Complaints • Divided loyalty with adult and child • Understanding that the harm was not deliberate • Losing control of the safeguarding process or lack of faith in it • Being adult focused
Case Study • Sisters Oluchi (9) and Ada (7) are brought to see you for their travel vaccinations for Nigeria. • They are both excited about going to buy special dresses to wear to a party at their grandmother’s. • What are you worried about? • What are you going to do?
Physical Neglect Observing or hearing reports of Scavenging, stealing or hiding food Poor hygiene that affects the child’s health Inadequate provision of food Living in an unsafe environment Other equally poor families manage better
Medical Neglect Use Was Not Brought not DNA https://www.youtube.com/watch?v=dAdNL6d4lpk • Not brought to appointments for immunisations or medication reviews • Not supervised using inhalers • Carers not interested in learning life support • Black or missing teeth
Subconjunctival Haemorrhage Lots of babies are referred because this is not properly documented at birth • Always check for SCH at birth visits and document this in the red book • Advise parents to take dated photos of all birthmarks and SCHs when they see them
Looked After Children • All of them are vulnerable by definition so be extra vigilant • Children can be taken into care by court order or voluntarily • Ask who has parental responsibility • Foster carers have delegated responsibility but parents should be involved in major decisions if there is time • Document the names and relationships of adults present • Read code the children and use the safeguarding template on S1 • Request records urgently and summarise them quickly • Check they have LAC medicals 6 monthly (under 5s) or yearly
Domestic Abuse Symptoms and signs Emotional or psychological symptoms Intrusive “others” in the consultation Primary Care Referral Pathway
Be part of the solution Contribute to child protection processes Review progress Communicate with colleagues about further concerns and escalate these if you do not feel you are being taken seriously • Attend or write letters for case conferences • Ensure you have received minutes and know what the plan is • Document this clearly according to guidelines