Download
1 / 30
300 likes | 374 Views
NEUTROPHIL GELATINASE-ASSOCIATED LIPOCALIN IS ELEVATED IN BILE FROM PATIENTS WITH MALIGNANT PANCREATOBILIARY DISEASE.

E N D
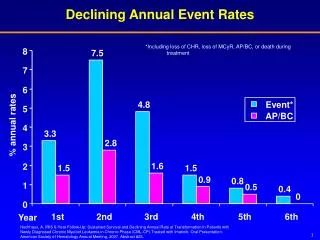
NEUTROPHIL GELATINASE-ASSOCIATED LIPOCALIN IS ELEVATED IN BILE FROM PATIENTS WITH MALIGNANT PANCREATOBILIARY DISEASE A. Zabron1, V. Horneffer-van der Sluis 2, C. Wadsworth 1, M. Gierula 2, A. Thillainayagam 3, P. Vlavianos3, D. Westaby 3, S. Taylor-Robinson 1, R. Edwards 2, S. Khan 1 1Hepatology and Gastroenterology Section, Division of Diabetes Endocrinology and Metabolism, Department of Medicine, 2Centre of Pharmacology and Therapeutics , Imperial College London,3Gastroenterology Unit , Hammersmith Hospital, Imperial College Healthcare NHS Trust, London, United Kingdom Previously presented at UEGW and BSG. Accepted for publication in the American Journal of Gastroenterology ACADEMIC TRAINEES ANNUAL EVENT 2011 sdfgafgafga
Content Focus on pancreatic adenocarcinoma Significance and current diagnostic difficulties Proteomic technique Results Possible clinical use and further work Summary
Pancreatic adenocarcinoma • Imperial AHSC HPB tertiary referral centre • 10th commonest cancer in the UK • Mortality similar to incidence • Diagnosis by cross-sectional imaging, histology / cytology and serum biomarkers imperfect • Frequently present with biliary obstruction
Bile as a diagnostic sample in malignant pancreatobiliary disease • Current cytological analysis of brushings – low sensitivity • Spy-glass • Metabonomic interest • Recent proteomic interest • IGF1 and pancreatic elastase-3B higher in CC bile (Alvaro D. et al., 2009) • CEACAM-6 and MUC1(CA 19-9) higher in PA bile (Farina et al., 2009)
Current Study • Aims: • To investigate the potential of bile as a source of novel biomarkers in pancreatic adenocarcinoma • Design: • Cohort study • Discovery phase - label-free proteomics to unfractionated sample, antibody-based techniques • Validation cohort
Sample collection and preparation • Bile aspirated at ERCP in patients with benign or malignant disease prior to introduction of contrast • Routine blood results/ serum markers, demographics etc recorded • Blood and urine collected at same event
Label-free proteomics: tryptic peptide production Crude centrifuged sample:water/ lipids/ bile acids and pigments/ proteins Pancreatic cancer Slice gel into equal fragments containing denatured proteins in size ranges No cancer SDS-PAGE Tryptic peptides In-gel protease digestion Extract from gel slice
Label-free proteomics: LC-MS/MS Peptide fragments Intensity of detection Retention time (min) Mass/carge ration (m/z) Retention time (min) Retention time (min)
Label-free proteomics: Normalisation and Quantification 1 11 18 Benign CC PaCa Mass/charge ration (m/z) Mass/charge ration (m/z) Mass/charge ration (m/z) VPLQQNFQDNQFQGK Retention time (min) Retention time (min) Retention time (min) “196,454.71” Normalised abundanceof aspecific protein in gel piece Progenesis, nonlinear dynamics Normalised abundance profileof single peptide spot Normalised abundance volume ofall peptide spots of an identified protein
Data analysis • SEQUEST • human RefSeq protein sequence database (NCBI) • Progenesis • Quantification by non-linear dynamics • Statistical analysis
Results of label-free proteomics • Bile analysed from patients with pancreatic adenocarcinoma (n=4) and benign biliary disease (n=4) • Over 200 different proteins identified including S100A6, LCN2, CEACAM6, REG1α, PRDX6 • 10 proteins varied significantly in abundance between benign and malignant groups
NGAL_HUMAN: Lipocalin 2 or Neutrophil gelatinase-associated lipocalin Normalised abundance volume ofall peptide spots of lipocalin 2 • P = 0.029, protein fold change 13.9 • 10 unique tryptic peptides • 52% protein sequence coverage
NGAL as a novel biomarker: Biological plausibility • “stress protein” • Novel urinary biomarker in for acute kidney injury • Overexpression in malignancy e.g. breast, ovarian, colon and pancreatic tissue
Western blot of NGAL in bile Gel 1 Gel 2 P<0.0001
ELISA of NGAL in different body fluids a) c) b) p=0.007 NS NS Bile Serum Urine
NGAL in bile as a diagnostic marker Receiver Operator Characteristics Area Under the Curve: 0.80
Combination of NGAL in bile and serum CA19-9 Cut-off NGAL in bile: 3000 ng/ml Cut-off serum CA19-9: 110 U/ml Sensitivity: 85% Specificity: 82% PPV: 79% NPV: 87%
Validation cohort Cut-off >570ng/ml gives sensitivity 100%, specificity 55%
Biological functions of NGAL in malignancy Schematic model of NGAL-mediated iron traffic. [Kai M. Schmidt-Ott et al. J Am Soc Nephrol 18: 407–413, 2007] A) B) Principal cellular mechanisms attributed to NGALin determining its pro- and anti-tumoral effects. [Bolignano D, et al. Cancer Lett. (2010) Vol. 288(1): pp 10-6.] General structure of A) the ferrichromes, prototypical hydroxamate type siderophores, and B) ferric enterobactin, a prototypical catechol-type siderophore. [Neilands J B, et al. J. Biol. Chem. 1995;270:26723-26726]
Summary • Valuable HPB patient cohort and scientific facilities available at Imperial AHSC • This study identified over 200 proteins in bile • Confirmed that proteomic analysis of body fluids allows identification of potential biomarkers in pancreatobiliary malignancy • There are significant differences in the proteome of bile in malignant and benign pancreatic disease
Summary 2 • This study highlights the increased abundance of bile LCN2/ NGAL in pancreatic adenocarcinoma. • Further work is required to elucidate the possible use of biliary LCN2/NGAL as a clinical marker of disease.
Future work • Increasing collaborations with Imperial HPB teams to expand recruitment • Validation of biliary NGAL as a diagnostic and/ or prognostic marker in pancreatic cancer • Exploration of its biological mechanism e.g. role stabilising MMP-9 • Extension of this approach to other biliary tract disease
Acknowledgements • British Liver Trust • Alan Morement Memorial Fund Patients! HPB and Endoscopy teams at Imperial AHSC Proteomics team at Imperial College