Download
1 / 1
10 likes | 78 Views
No. 208. Intravesical BCG for patients with N on M uscle I nvasive Bladder C ancer (NMIBC): Do local results reflect those in the published literature?. Bushra Othman 1 , Daniel Steiner 2 , Sue Wallace 3 , Tania Hossack 4 , Douglas Travis 5 .

E N D
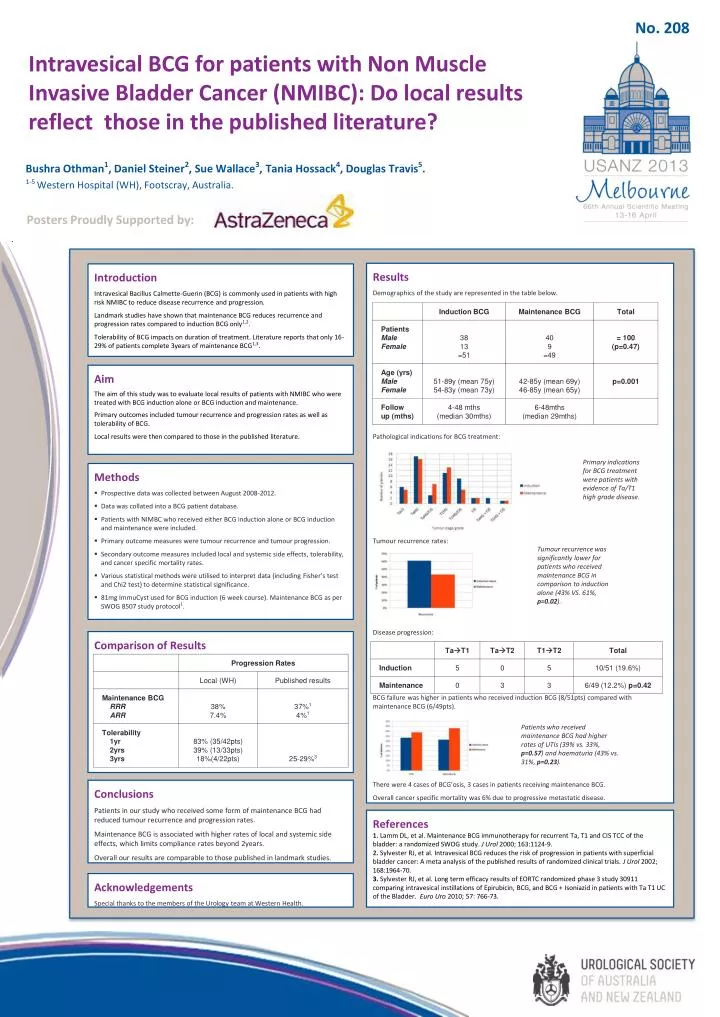
No. 208 Intravesical BCG for patients with Non Muscle Invasive Bladder Cancer (NMIBC): Do local results reflect those in the published literature? Bushra Othman1, Daniel Steiner2, Sue Wallace3, Tania Hossack4, Douglas Travis5. 1-5 Western Hospital (WH), Footscray, Australia. Posters Proudly Supported by: Results Demographics of the study are represented in the table below. Pathological indications for BCG treatment: Tumour recurrence rates: Disease progression: BCG failure was higher in patients who received induction BCG (8/51pts) compared with maintenance BCG (6/49pts). There were 4 cases of BCG’osis, 3 cases in patients receiving maintenance BCG. Overall cancer specific mortality was 6% due to progressive metastatic disease. Introduction Intravesical Bacillus Calmette-Guerin (BCG) is commonly used in patients with high risk NMIBC to reduce disease recurrence and progression. Landmark studies have shown that maintenance BCG reduces recurrence and progression rates compared to induction BCG only1,2. Tolerability of BCG impacts on duration of treatment. Literature reports that only 16-29% of patients complete 3years of maintenance BCG1,3. Aim The aim of this study was to evaluate local results of patients with NMIBC who were treated with BCG induction alone or BCG induction and maintenance. Primary outcomes included tumour recurrence and progression rates as well as tolerability of BCG. Local results were then compared to those in the published literature. Primary indications for BCG treatment were patients with evidence of Ta/T1 high grade disease. • Methods • Prospective data was collected between August 2008-2012. • Data was collated into a BCG patient database. • Patients with NIMBC who received either BCG induction alone or BCG induction and maintenance were included. • Primary outcome measures were tumour recurrence and tumour progression. • Secondary outcome measures included local and systemic side effects, tolerability, and cancer specific mortality rates. • Various statistical methods were utilised to interpret data (including Fisher’s test and Chi2 test) to determine statistical significance. • 81mg ImmuCyst used for BCG induction (6 week course). Maintenance BCG as per SWOG 8507 study protocol1. Tumour recurrence was significantly lower for patients who received maintenance BCG in comparison to induction alone (43% VS. 61%, p=0.02). Comparison of Results Patients who received maintenance BCG had higher rates of UTIs (39% vs. 33%, p=0.57) and haematuria (43% vs. 31%, p=0.23). Conclusions Patients in our study who received some form of maintenance BCG had reduced tumour recurrence and progression rates. Maintenance BCG is associated with higher rates of local and systemic side effects, which limits compliance rates beyond 2years. Overall our results are comparable to those published in landmark studies. References 1.Lamm DL, et al. Maintenance BCG immunotherapy for recurrent Ta, T1 and CIS TCC of the bladder: a randomized SWOG study.J Urol2000; 163:1124-9. 2.Sylvester RJ, et al. Intravesical BCG reduces the risk of progression in patients with superficial bladder cancer: A meta analysis of the published results of randomized clinical trials. J Urol2002; 168:1964-70. 3. Sylvester RJ, et al. Long term efficacy results of EORTC randomized phase 3 study 30911 comparing intravesical instillations of Epirubicin, BCG, and BCG + Isoniazid in patients with Ta T1 UC of the Bladder. Euro Uro2010; 57: 766-73. Acknowledgements Special thanks to the members of the Urology team at Western Health.






