Download
1 / 39
410 likes | 509 Views
Explore the latest findings in pediatric aspergillosis and unique perspectives on its management. Learn from clinical trials and epidemiological studies on this invasive fungal infection affecting children. Stay informed with expert analysis and treatment updates.

E N D
Pediatric Aspergillosis:New Findings and Unique Aspects William J. Steinbach, MD Assistant Professor of Pediatrics, Molecular Genetics, and Microbiology Pediatric Infectious Diseases Duke University Medical Center
Randomized Clinical Trials for Invasive Aspergillosis • Voriconazole vs. AmB-deoxycholate • 277 patients; Eligible patients 12 years old • Voriconazole MITT mean age 48.5 yrs (13 - 79 yrs) • AmB MITT mean age 50.5 yrs (12 - 75 yrs) Herbrecht R, et al. New Engl J Med 2002;347:408-15. • ABCD vs. AmB-deoxycholate • 174 patients; Eligible patients > 2 years old • ABCD mean age 48 yrs (7 - 81 yrs) • AmB mean age 44 yrs (0 - 81 yrs) Bowden R, et al. Clin Infect Dis 2002;35:359-66.
Other Invasive Aspergillosis Clinical Trials • MSG Multicenter Itraconazole • 76 patients; No age eligibility restriction • Pulmonary disease mean age 47.5 yrs • Extrapulmonary disease mean age 48.9 yrs Denning DW, et al. Am J Med 1994;97:135-144. __________________________________________________________________________________________________________ • Two doses of L-AmB • 87 patients; Eligible patients > 1 year old • L-AmB (1 mg/kg/d) mean age 51 yrs (14 - 74 yrs) • L-AmB (4 mg/kg/d) mean age 46 yrs (15 - 81 yrs) Ellis M, et al. Clin Infect Dis 1998;27:1406-12. __________________________________________________________________________________________________________ • Efficacy and Safety of Voriconazole • 116 patients; Eligible patients 14 years old • Mean age 52 yrs (18 - 79 yrs) Denning DW, et al. Clin Infect Dis 2002;563-71.
Treatment Practices in Invasive Aspergillosis • Treatment Practices and Outcomes • 595 Patients • Mean age 42.3 yrs (0 - 86 yrs) Patterson TF, et al. Medicine 2000;79:250-60. • EORTC Diagnosis and Therapeutic Outcome • 123 patients • Mean age 46 yrs (9 - 83 yrs) Denning DW, et al. J Infect 1998;37:173-80.
Epidemiology of Invasive Aspergillosis • Risk Factors for mould infection in BMT patients • Infected (n=21) mean age 29 yrs (1 - 43 yrs) • Uninfected (n=209) mean age 28 yrs (0.25 - 54 yrs) Yuen K-Y, et al. Clin Infect Dis 1997;25:37-42. ________________________________________________________________________________________________ • Invasive aspergillosis in greater Paris area • 621 patients • Mean age 40.3 yrs (6 days – 89.7 yrs) Cornet M, et al. J Hosp Infect 2002;51:288-96. _______________________________________________________________________________________________ • Early infections in HSCT • 409 patients • Mean age 32 yrs (6mo – 65 yrs) Kruger W, et al. Bone Marrow Transplant 1999;23:589-597. __________________________________________________________________________________________________________________ • Allogeneic HSCT after non-myeloablative conditioning • 173 patients • Mean age 53 yrs (0 - 72 yrs) Fukuda T, et al. Blood 2003;102:827-33.
Epidemiology of Invasive AspergillosisStratified by Age • FHCRC; 1985-1999 • 327 patients with Proven / Probable IA • < 19 years 39 cases (13%) • 19-40 years 99 cases (34%) • > 40 years 156 cases (53%) • No mention of # of HSCT divided by age, so cannot determine incidence inside age range Marr KA, et al. Clin Infect Dis 2002;34:909-17.
Invasive Aspergillosis in Pediatric HSCT • 1986-1996; 148 pediatric HSCT patients • Mean ages • Autologous 7.1 yrs (1.0 - 17 yrs) • Allogeneic 7.7 yrs (0.6 - 17 yrs) • 8 patients with proven invasive aspergillosis • Allogeneic (6/73; 8%) • Autologous (2/75; 3%) • 48 patients with suspected IFI not separated between Candida and Aspergillus • No IA specific analyses Hovi L, et al. Bone Marrow Transplant 2000;26:999-1004.
Invasive Aspergillosis in Pediatric HSCT • 510 HSCT in 485 patients (1990-1998) • Birth – 21 years old • 584 culture-proven infections in first year post-transplant • 26 Invasive aspergillosis cases (4.5% of infections) • IA post-transplant days • 0-30 n=10 • 31-100 n=13 • 101-365 n=3 • In multivariable analysis IA more likely to have severe GVHD (RR 7.5; 95% CI 3.0-18.4) Benjamin DK Jr., et al. Pediatr Infect Dis J 2002;21:227-34.
Invasive Aspergillosis Autopsy by AgeData from 1989, 1993, 1997 Age Range (yrs)MaleFemale 0 - 9 11 3 10 - 19 21 3 20 - 29 12 6 30 - 39 27 6 40 - 49 33 17 50 - 59 60 32 60 - 69 67 35 70 - 79 40 29 > 80 8 2 Total 279 133 Kume H, et al. Pathol Intl 2003;53:744-50.
Age (yrs) No. ofpatients No. ofdeaths CFR, % 20 22 15 68.2 21 - 30 27 16 59.3 31 - 40 52 31 59.6 41 - 50 57 30 52.6 51 - 60 49 29 59.2 > 60 31 17 54.8 Unreported 135 76 56.3 IA Case Fatality Rate by Age 1,941 patients in case series after 1995 Mean age 44.2 yrs (3-91 yrs) “There was little variation in mortality by age.” Lin S-J, et al. Clin Infect Dis 2001;32:358-66.
Hospital for Sick Children, Toronto • 39 IA Cases; 1979 – 1988 • 24 Proven, 15 Probable IA • Median age 10 years (22 days -18 years) • 74% with hematologic malignancy or BMT recipient • 31/36 patients with ANC < 500 at diagnosis • Mean duration of ANC < 1000 was 20 days • Hospitalized for a mean of 47 days (0-180) in 6 months preceding diagnosis • Survival 23.1% (9/39) Walmsley S, et al. Pediatr Infect Dis J 1993;12:673-82.
Hospital for Sick Children, Toronto • Cutaneous • 41% (16/39) cases first suspected as a skin lesion • Skin lesion resolved in 56% (9/16) and in all coincident with neutropenic recovery; others died • Pulmonary • 41% (16/39) cases first suspected as a fever with abnormal CXR or chest pain • 94% died, the one survivor had neutropenic recovery Walmsley S, et al. Pediatr Infect Dis J 1993;12:673-82.
Species Distribution:Pediatric SpeciesToronto1 (n=26 isolates) A. fumigatus 4 A. flavus 17 A. niger 1 A. nidulans 1 A. terreus 3 1 Walmsley S, et al. Pediatr Infect Dis J 1993;12:673-82.
Species Distribution:Pediatric vs. Adult SpeciesToronto1BAMSG2 (n=26 isolates) (n=256 isolates) A. fumigatus 4 171 (67%) A. flavus 17 41 (16%) A. niger 1 14 (5%) A. nidulans 1 2 (5%) A. terreus 3 8 (3%) 1 Walmsley S, et al. Pediatr Infect Dis J 1993;12:673-82. 2 Perfect JR, et al. Clin Infect Dis 2001;33:1824-33.
St. Jude Children’s Hospital • 1962-1996; 9,500 children treated • 66 cases of proven IA (0.7 % incidence) • Median age 11.2 yrs (1.3 – 21.6 yrs) • ANC < 500 duration for median 14 days (1-402 days) • Onset of underlying disease and IA was median 16 months (0- 180 months) • 44 (66%) hospitalized for median of 36 days (1-52 days) before onset of clinical disease • Clinical symptoms median 11 days (0-69 days) before diagnosis of IA Abassi s, et al. Clin Infect Dis 1999;29:1210-9.
Incidence of Proven Invasive Aspergillosis:St. Jude Children’s Hospital • MDS 8% (2/25) • CGD 7% (1/14) • Choriocarcinoma 6% (1/16) • Aplastic anemia 4.6% (2/43) • AML 4% (26/647) • CML 4% (1/24) • ALL 1% (29/2659) • Neuroblastoma 0.17% (1/583) • Lymphoma 0.16% (2/1188) Abassi s, et al. Clin Infect Dis 1999;29:1210-9.
St. Jude Children’s Hospital • Survival of 15% at one year • End of 1 month 58% survival • End of 2 months 25% survival • End of 10 months 15% survival • Pulmonary disease fared worse than those without pulmonary disease • Median time between diagnosis and death was 29 days (3-312 days) Abassi s, et al. Clin Infect Dis 1999;29:1210-9.
Pediatric Culture Location LocationToronto1St. Jude2 (n=39) (n=66) Lung 10 31 Sinus / Nose 0 11 Skin 15 12 Tracheal 1 6 Blood 0 4 Bone 0 2 Heart/Pericardial fluid 0 2 Brain 2 2 Eye 0 2 Pleural fluid 0 1 CSF 0 1 Liver / Kidney 0 2 Esophagus / Bowel 2 0 Disseminated 9 0 1 Walmsley S, et al. Pediatr Infect Dis J 1993;12:673-82. 2 Abassi s, et al. Clin Infect Dis 1999;29:1210-9.
Species Distribution:Pediatric vs. Adult SpeciesSt. Jude1Toronto2BAMSG3 (n=39) (n=26) (n=256) A. fumigatus 15 4 171 A. flavus28 17 41 A. niger 0 1 14 A. nidulans 1 1 2 A. terreus 5 3 8 Other Aspergillus 0 0 0 1 Abassi s, et al. Clin Infect Dis 1999;29:1210-9. 2 Walmsley S, et al. Pediatr Infect Dis J 1993;12:673-82. 3 Perfect JR, et al. Clin Infect Dis 2001;33:1824-33.
Species Distribution:Pediatric vs. Adult SpeciesSt. Jude1Toronto2BAMSG3 VCZ4 (n=39) (n=26) (n=256) (n=110) A. fumigatus 15 4 171 85 A. flavus28 17 41 7 A. niger 0 1 14 9 A. nidulans 1 1 2 1 A. terreus 5 3 8 6 Other Aspergillus 0 0 0 2 1 Abassi s, et al. Clin Infect Dis 1999;29:1210-9. 2 Walmsley S, et al. Pediatr Infect Dis J 1993;12:673-82. 3 Perfect JR, et al. Clin Infect Dis 2001;33:1824-33. 4 Herbrecht R, et al. New Engl J Med 2002;347:408-15.
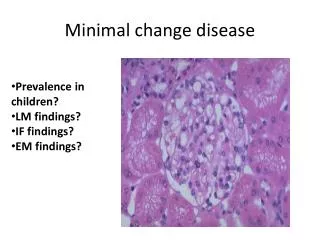
Neonatal Aspergillosis • Invasive candidiasis much more common • In neonates, IA is more primary cutaneous • Age of onset early, can be soon after birth • Risk factors • Immature phagocytes • Corticosteroids • Prolonged hospitalization • Skin trauma • Tape adhesive / removal from immature thin skin • Macerated skin due to prolonged arm boards
Neonatal Primary Cutaneous Aspergillosis – Buttocks lesion Woodruff CA, et al. Pediatr Dermatol 2002;5:439-44.
Neonatal Aspergillosis • Review of 44 cases in first 90 days of life • Primary cutaneous (25%; n=11) • Invasive pulmonary (22.7%; n=10) • CNS (9.1%; n=4) • Gastrointestinal (6.8%; n=3) • Misc. single site (4.5%; n=2) • Disseminated (31.8%; n=14) Groll AH, et al. Clin Infect Dis 1998;27:437-52.
Neonatal Aspergillosis ConditionTotalCutaneousPulmonaryDisseminated (n=44) (n=11) (n=10) (n=14) Prematurity 43.2% 90.9% 20% 28.6% CGD 13.6% 0 50% 7.1% Prior neutropenia 2.3% 0 0 7.1% Groll AH, et al. Clin Infect Dis 1998;27:437-52.
Species Distribution SpeciesNeonatal1St. Jude2Toronto3BAMSG4 (n=44) (n=39) (n=26) (n=256) A. fumigatus18 15 4 171 A. flavus 6 28 17 41 A. niger 3 0 1 14 A. nidulans 0 1 1 2 A. terreus 0 5 3 8 Other Aspergillus 5 0 0 0 N/A 12 0 0 0 1 Groll AH, et al. Clin Infect Dis 1998;27:437-52. 2 Abassi s, et al. Clin Infect Dis 1999;29:1210-9. 3 Walmsley S, et al. Pediatr Infect Dis J 1993;12:673-82. 4 Perfect JR, et al. Clin Infect Dis 2001;33:1824-33.
ABLC in Adults and Children:Open-Label Use • 1990-1995; ABLC given for proven/probable IFI • All patients analyzed • 556 cases, 291 evaluable for efficacy • Overall mean age 37.2 yrs (21 days – 93 years) • 130 cases of IA (CR + PR = 42%) Walsh TJ, et al. Clin Infect Dis 1998;26:1383-96. • Patients < 18years old • 111 treatment episodes of pediatric IFI • 54 evaluated for efficacy • Overall median age 11 years (21 days – 16 years) • 25 cases of IA (CR + PR = 56%) Walsh TJ, et al. Pediatr Infect Dis J 1999;18:702-8.
Comparison Adult vs. Pediatric Outcomes Ages CR + PR CR PR Stable Failure All (n=130)1 42% 17% 25% 12% 45% Pulm (n=74) 38% 9% 28% 16% 46% Diss (n=27) 30% 15% 15% 11% 59% Sinus (n=14) 64% 36% 29% 7% 29% Single (n=15) 67% 40% 27% 0 33% Peds (n=25)2 56% 28% 28% 8% 36% Pulm (n=10) 50% 20% 30% 10% 40% Diss (n=7) 29% 14% 14% 14% 57% Sinus (n=5) 100% 60% 40% 0 0 Single (n=3) 67% 33% 33% 0 33% 1 Walsh TJ, et al. Clin Infect Dis 1998;26:1383-96. 2 Walsh TJ, et al. Pediatr Infect Dis J 1999;18:702-8.
Voriconazole for Pediatric Aspergillosis • Compassionate Use; 58 IFI including 42 IA • Mean age 8.2 yrs (9 mo – 15 yrs) • Therapeutic response • Complete or partial response 43% • Pulmonary IA (n=12) 33% • CNS (n=6) 50% • Disseminated (n=7) 86% • Sinusitis (n=7) 29% • Bone / Liver / Skin (n=10) 30% • Stable 7% • Intolerance 10% • Failure 40% Walsh TJ, et al. Pediatr Infect Dis J 2002;21:240-8.
Phase II Micafungin:Monotherapy or Combination • Failing, likely to fail, or intolerant of OLT • 283 patients enrolled • Mean age 37 yrs (9 wks – 84 yrs) • 63 (22.3%) were < 16 yrs • Median duration of therapy • Adults 34 days • Children 37 days • Hope to see pediatric-specific outcome data Ullman AJ, et al. ECCMID 2003, Abstract O-400
Pediatric Radiology • 27 consecutive patients; 10 yr review • Mean age 5 yrs (7 mo – 18 yrs) • In adult series, approx. 50% with cavitation and air crescent formation in 40% • Central cavitation of small nodules in 25% children • No evidence of air crescent formation within any area of consolidation on CT Thomas KE, et al. Pediatr Radiol 2003;33:453-60. • Other pediatric series (higher mean ages): • 22% (6/27) with cavitation on CXR Allan BT, et al. Pediatr Radiol 1988;18:118-22. • 43% (6/14) with cavitation on CT Taccone A, et al. Pediatr Radiol 1993;23:177-80.
Galactomannan Assay • Prospective study from 1995-1998 • 450 adult allogeneic HSCT patients (3883 samples) • 347 children with hematologic malignancies (2376 samples) • First positive results • Adult patients: median of 74 days post-transplant • Pediatric patients: median of 36 days Sulahian A, et al. Cancer 2001;91:311-8.
Galactomannan Assay • False-positive antigenemia • Adult patients 2.5% (10/406) • Pediatric patients 10.1% (34/338) • GM > 1.5 in at least two sequential samples AdultPediatric • Sensitivity 88.6% 100% • Specificity 97.5% 89.9% • If the lower cut-off was lowered 1.0, the pediatric specificity was even lower at 88.1%. Sulahian A, et al. Cancer 2001;91:311-8.
Galactomannan Assay • 797 episodes (inc. 48 pediatric patients) • FUO group, false-positives: • Adults (0.9%) vs. Children (44.0%) (p < 0.0001) • Overall specificity: • Adults (98.2%) vs. Children (47.6%) (p < 0.0001). • Overall positive predictive value: • Adult nonallogeneic HSCT recipients (92.1%) • Adult allogeneic HSCT patients (42.9%) • Children (15.4%) (p < 0.0001) Herbrecht R, et al. J Clin Oncol 2002;20:1898-1906.
GM Cross-Reactivity • Membrane-associated molecule of Bifidobacterium bifidum spp. pennsylvanicum found to mimic the epitope recognized by EB-A2 and cultures showed in vitro reactivity with Aspergillus sandwich ELISA Mennink-Kersten M, et al. Lancet 2004;363:325-7. • Bifidobacterium spp. common in gut microflora • Breast-fed neonates 91% total microflora • Formula-fed neonates 75% total microflora • 8/14 milk formulas tested were positive for GM • All breast milk samples were negative for GM Warris A, et al. ICAAC 2001, Abstract J-848.
Collaborative Pediatric Groups There has never been a large scale dedicated pediatric invasive aspergillosis study for diagnosis or treatment • Children’s Oncology Group (USA) • BFM (Germany)
Pediatric Differences? • Potential Aspergillus species differences • Radiologic differences • Less cavitation on CT • Cutaneous presentation • 89 cases reviewed, 63% (56/89) in children Walmsley S, et al. Pediatr Infect Dis J 1993;12:673-82. • Avoid armboards or change frequently • Galactomannan sensitivity / false-positivity • Antifungal PK, dosing, and efficacy? • Combination Therapy • Less reported, could be different