Download
1 / 68
710 likes | 1.02k Views
Multidisciplinary Management of Squamous Cell Esophageal Cancers. Case presentations & treatment perspectives from Gastroenterology Radiation Oncology, Surgical Oncology, and Medical Oncology. Learning Objectives:. After attending this session, the participants should be able to:

E N D
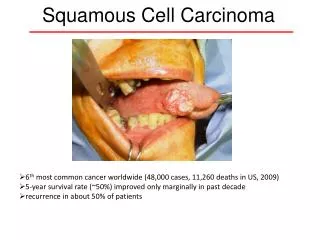
Multidisciplinary Management of Squamous Cell Esophageal Cancers Case presentations & treatment perspectives from Gastroenterology Radiation Oncology, Surgical Oncology, and Medical Oncology
Learning Objectives: After attending this session, the participants should be able to: • Identify current controversies in the management of patients with localisedsquamous cell cancer of the esophagus • Discuss state-of-the art treatment options for patients esophageal squamous cell cancers
Session Outline: • Case 1: T3N2M1 (cervical lymph node) squamous cell carcinoma • Case 2: T3N1M0 squamous cell carcinoma in a comorbid patient
Perspectives: • Radiation Oncology: Lawrence R. Kleinberg, Johns Hopkins University • Surgery: Joe B. Putnam, Vanderbilt University • Medical Oncology: Michael Stahl, Kliniken Essen-Mitte • Gastroenterology: Mouen A. Khashab, Johns Hopkins University
Case 1: • 66 yearold man, still workingas a physician in practice, ECOG 0, peripheralarterialocclusivedisease (recentlystenting of A. iliacacom.), normal liverandrenalfunction • EGD: • Obstructing tumor 29-35cm from the incisors • Polypoid lesion • Normal gastric exam • Histology: squamous cell carcinoma
Case 1: (cont.) • Endosonography Removal of all layers of esophageal wall. Enlarged regional lymph nodes 21.2 mm • Bronchoscopy • No infiltration or impression of the tracheo-bronchial tree 15.4 mm
Case 1: (cont.) • PET-CT • primarycanceroftheesophagus, length 7 cm (SUV 16.5), • 3 nodes in theuppermediastinum (SUV 3.0 – 6.1) • Rightcervicalnode of 6.1 cm3volume (SUV 16.5) • uT3 N2 M1 (lymph)
Case 1: T3 N2 M1 (cervical lymph node) • Gastroenterology Perspective on diagnosis:
Audience Question (1) What is your recommendation for initial treatment of this 66 year old patient with a T3N2M1 (cervical lymph node metastasis) SCC of mid esophagus? • Neo-adjuvant chemoradiotherapy planned Surgery (three field lymphadenectomy) • Induction chemotherapy Chemoradiotherapy Surgery only in case of tumor response • Definitive chemoradiotherapy including cervical nodes • Palliative chemoradiotherapy of primary esophagealtumor • Surgery Chemo-RT
Case 1: T3 N2 M1 (cervical lymph node) Answers from the audience to question 1
Audience Question (2) After radiochemotherapy (50.4 Gy + weekly cisplatin-based chemotherapy) with almost complete response what would be your next recommended step • Surgery with three field lymphadenectomy • Increasing radiation dose to 66 Gy, including the cervical nodes • Completion of chemotherapy up to 4 - 6 courses • Wait and see
Case 1: T3 N2 M1 (cervical lymph node) Answers from the audience to question 2
RADIOTHERAPY QUESTION Randomized Trials Have Established Trimodality Therapy as a Standard Compared with Surgery Alone Is concurrent chemoradiation a valid alternative to surgical management?
Chemoradiotherapy Alone Valid Option for Squamous Cell Carcinomas Squamous Cell Sites Effective Organ Preserving Curative Therapy for Squamous Cell Adenocarcinoma ChemoRT Not Effective Option for Local Control Parotid Pancreas Colon Rectum • Oropharynx • Larynx • Oral Cavity • Anal • Esophagus?
Radiochemotherapy: Curative For Esophageal Squamous Cell Carcinoma?
Why Consider Adding Surgery? Responders to chemoradiation Randomized +/- surgery All Enrolled Patients Randomized +/- Surgery 2 Year Local Control 66% vs. 57% Stent Placement 5% vs. 32% 3 month death 9.3% vs 0.8% 2 year Local PFS 64% vs. 41% Treatment Death 12.8% vs. 3.5% Bedenne L et al. JCO 2007;25:1160-1168 Stahl M et al. JCO 2005;23:2310-2317
Is data for chemoradiation as a viable alternative still valid today? Questions Exist • The competing risks that prevent a benefit may be less important in current area • Only those who survive surgery: Mortality decreased in recent trials. • “CROSS” Trial: 6% 30 day post-op mortality • ECOG 1201: 3% 30 day post-op mortality • Only those without metastasis at time of treatment can benefit. Better staging today with PET, CT scanning. • More successful systemic therapy may increase importance of local control for survival. • Better ability to select responders may be important.
When Should Surgery be Added?Issue Remains Controversial. • All appropriate surgical candidates for local control benefit? • All appropriate surgical candidates as benefits may be greater now with decreased mortality and more accurate staging? • In clinical trials to better assess new systemic therapies with reduced competing risk of local progression? • PET Guided Assessment of Response to ChemoRT in Future? • SUV decline >51% after PET 4-5 weeks/6-7 weeks RT • Hazard ratio for death 0.331 • Median Survival 37 vs. 19 months • 5 Year survival 40% vs. 0% • Yang ClinNucl Med 2011;36: 860–866 • CT Scan/EUS Unreliable at assessing response
Case 1: T3 N2 M1 (cervical lymph node) • Surgery Perspective: Joe B. Putnam, MD; Vanderbilt University, Nashville, Tennessee • Esophagectomy in the presence of extrathoracic nodal metastases is not standard. • If palliation of dysphagia has occurred, then the role of surgery would be supportive only. • If recurrence, endoscopy and stent placement could be considered
Case 1: T3 N2 M1 (cervical lymph node) • Radiation Oncology Perspective:
Case 1: T3 N2 M1 (cervical lymph node) Data-drivenstaging fortheseventhedition of the AJCC / UICC stagingmanuals Stage IV Rice TW, Cancer 116:3763, 2010
Case 1: T3 N2 M1 (cervical lymph node) • Medical Oncology Perspective: M. Stahl, Kliniken Essen-Mitte, Essen, Germany • We must reflect that patients with distant lymph node metastases can only be treated with palliative intent • So, palliative chemotherapy and best supportive care are indicated • Special focus should be kept on sustaining the capability to swallow
Case 1: T3 N2 M1 (cervical lymph node) What is your recommended treatment for this 66 year old patient with a T3N2M1 (cervical lymph node metastasis) SCC of mid esophagus? Answers from the audience to question 2
Radiotherapy Question Should patients with cervical and supraclavicular disease be treated for cure?
Should Deep Cervical/Supraclivicular Nodes be Irradiated? Lymph Flow Esophageal Cancer Incidence of Cervical Nodes Squamous cell clinical and imaging positive cervical nodes*, 1017 pts Upper third 17% Middle third 4% Lower third 2% Subclinical Cervical Nodes** Aggregate analysis 18,415 pts. 3 Field dissection Upper third 30% Middle third 17% Lower third 11% *Huang, Rad and Oncol 95: 2010; 229–233 **Ding, Br J Radiol. 2012 85: 1110-9 Nishira, Surg Today (1995) 25:307-317
Cervical (Deep Cervical and Supraclavicular) Nodes Curable?Selected cases; Some example reports
Case 1: T3 N2 M1 (cervical lymph node) What actually happened?
Case 1: T3 N2 M1 (cervical lymph node) The patient received 2 cycles of 6 weeks of induction chemotherapy (cisplatin, 5-FU, folinic acid) CT scan: After Induction Chemotherapy Esophagealtumorregressing (lenght 4 cm) Thickendesophageal wall up to 12.3 mm
Case 1: T3 N2 M1 (cervical lymph node) • Combined radiochemotherapy was initiated • The patient (orthopedic surgeon) demanded surgery • In our center we advised him against surgery • The patient was sent to a surgical high volume center in Germany • There surgery was also regarded as not indicated • The patient decided to complete definitive radiochemotherapy as planned
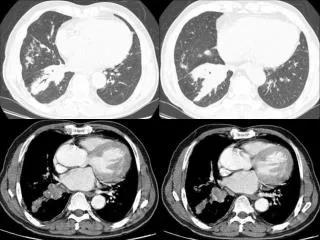
Case 1: T3 N2 M1 (cervical lymph node) The patient received Radiochemotherapy of the esophagus (66 Gy + weekly application of cisplatin / irinotecan, 50 Gy to the cervical nodes) CT scan: After Radio-Chemotherapy Esophagealtumoratandbelow thebifurcation (6 cm in length) Thickendesophageal wall up to 16.7 mm. Nomoreenlargedlymphnodes (also in cervicalregion). Nomets
Case 1: T3 N2 M1 (cervical lymph node) CT scan: After Radio-Chemotherapy Rapidly progressive dyspnoe overthe last days. Diffuse interstitialopacities in all lobes, suggestingatypicalpneumonia
Case 1: T3 N2 M1 (cervical lymph node) Endoscopy: After Radio-Chemotherapy Was not performed due to severe dyspnoe. Instead patient was admitted to the hospital and Antibiotic + antimykotic therapy was initiated
Audience Question (3) After having completed definitive radiochemotherapy how do you follow-up the patient? • X-ray and abdominal ultrasound only • CT-scan every 3 – 6 months • PET-scan every 3 – 6 months • No follow-up, just wait for symptoms
Case 1: T3 N2 M1 (cervical lymph node) Answers from the audience to question 3
Case 1: T3 N2 M1 (cervical lymph node) Audience questions for panel
Case 2: • 61 yearoldpatient, ECOG 1, COPD, GOLD group B (pink puffer), coronaryheartdiseasewithoutcardiacinfarction, normal liverand renal function • EGD: • Obstructing tumor 26-31cm from the incisors • ulcerous lesion • Normal gastric exam • Histology: squamous cell carcinoma
Case 1: (cont.) • Endosonography • Removal of all layers of esophageal wall. At lease 3 enlarged regional lymph nodes • Bronchoscopy • Impression of dorsal wall of trachea without infiltration
Case 1: (cont.) • PET-CT • primarycancer of theesophagus, length 6 cm (SUV 12.5) • 2 regional lymphnodes (SUV 4.0 – 7.0) • uT3 N1 M0
Case 2: T3 N1 M0 • Gastroenterology Perspective on diagnosis:
Audience Question What is your recommended treatment for this 61 year old somewhat comorbid patient with a T3N1M0 SCC of upper esophagus? • Neo-adjuvant chemoradiotherapy planned Surgery • Neoadjuvantchemoradiotherapy Surgery only in case of tumor response • Neoadjuvantchemoradiotherapy Salvage Surgery in case of residual tumor • Definitive chemoradiotherapy without surgery
Audience Question (??) What if the same patient will not show any tumor response to radiochemotherapy, but still may have localised EC? • Early salvage surgery with curative intent • Increasing radiation dose to 66 Gy to prolong time to local tumor progression • Consolidation chemotherapy to prolong time to progression? • Wait and see
Case 2: T3 N1 M0 (mid esophagus) • Surgery Perspective: Joe B. Putnam, MD; Vanderbilt University, Nashville, Tennessee • Staging of middle third esophageal tumors must include bronchoscopy • Esophagectomy can be performed safely following neoadjuvant chemoradiotherapy. Typical dose in the United States is 50.4 Gy • Neoadjuvant chemoradiotherapy is associated with R0 resection • R0 resection is associated with improved survival. • The decision for resection is made by the surgeon based on a multidisciplinary group discussion, and prior to the initiation of any therapy. • Resection is not performed if extra-regional metastases are confirmed.
Locally Advanced Disease • Dedicated multidisciplinary esophageal conference • Esophageal cancer • Benign esophageal diseases • Clinical services involved include: • Thoracic Surgery • General Surgery • GI Medical Oncology (specialist in GI, esophageal cancer) • GI Radiation Oncology • Pathology • Gastroenterology (experts in esophageal diseases, EUS with FNA, ablation techniques, GERD and motility studies) • Speech pathology
Long-term survival improves with R0 resection and preop chemoradiotherapy Treatment outcomes of resected esophageal cancer. Hofstetter W, et al. Annals of Surgery (2002) 236:376-84
Case 2: T3 N1 M0 (mid esophagus) • Radiation Oncology Perspective:
Case 2: T3 N1 M0 (mid esophagus) • Medical Oncology Perspective: M. Stahl, Kliniken Essen-Mitte, Essen, Germany • Based on a couple of meta-analyses trimodal therapy is regarded as standard treatment for locally advanced esophageal cancer • Patient selection is crucial due to high probability of postoperative mortality after radiochemotherapy • Definitive radiochemotherapy is an option for patients with increased operative risk • Early salvage surgery should be included in the treatment plan for patients with incomplete tumor response
CRT+S vs S aloneMeta-Analysis – 30-day mortality after S N = 509 vs 510 HR = 1.46 (0.91 – 2.33) Kranzfelder M, Br J Surg 98:768-83, 2011