Download
1 / 13
150 likes | 477 Views
COPD Exacerbations. UCI Internal Medicine Mini-Lecture Slideset updated 12/03/2012 by Michael Rochon -Duck. A Tale from the ED.

E N D
COPD Exacerbations UCI Internal Medicine Mini-Lecture Slideset updated 12/03/2012 by Michael Rochon-Duck
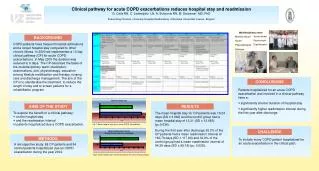
A Tale from the ED “I have an easy admission for you. 70-year-old active smoker with severe COPD, progressively short of breath for three days. Frequent flyer, was here last month with the same complaints. He’s afebrile and tachypneic, with wheezes and poor air movement on both sides. His chest film shows bilateral pneumonia, so I started ceftriaxone and azithromycin. I gave him Solumedrol and nebs, and he looks a little better.”
Objectives • Formulate a differential and workup for an acutely dyspneic patient with COPD • Choose appropriate initial therapy and anticipate complications • Plan for discharge to reduce readmissions
Precipitants of Exacerbation Acute bronchitis caused by: • Viruses • H. influenzae • Moraxella catarrhalis • Strep. pneumoniae • P. aeruginosa Three other potentially fatal precipitants: • Heart failure • Pneumonia • Pulmonary embolism
Initial Interventions • Bronchodilators: Duoneb q4h scheduled around-the-clock. • Steroids: oral prednisone (after first dose IV Solumedrol in ED) if the patient can swallow. Check fingerstick blood sugars. • Oxygen: caution! Titrate to SaO2 90-93% in advanced COPD to avoid hypercapneic respiratory failure • Antibiotics …
Consider Ventilation For … • Intractable dyspnea • Worsening hypercapnea • Refractory hypoxia
Discharge Planning • Optimize the patient’s inhaler regimen • Assess eligibility for home oxygen and pulmonary rehabilitation • Smoking cessation • Followup with PCP in 10-14 days
A Tale from the ED, Revisited “I have an easy admission for you. 70-year-old active smoker with severe COPD, progressively short of breath for three days. Frequent flyer, was here last month with the same complaints. He’s afebrile and tachypneic, with wheezes and poor air movement on both sides. His chest film shows bilateral pneumonia, so I started ceftriaxone and azithromycin. I gave him Solumedrol and nebs, and he looks a little better.”
Summary • Think of heart failure, pneumonia, and pulmonary embolism in the differential of all cases of COPD exacerbation (although viral respiratory infections are more common) • Treat with bronchodilators, systemic glucocorticoids, oxygen, and antibiotics • Reevaluate diagnosis and consider ventilation for declining respiratory status