Download
1 / 27
340 likes | 1.25k Views
Management of senile cataract. Surgical by cataract extraction surgery. CATARACT SURGERY. ● Indications ● Techniques ● Complications. Indications Of Cataract Surgery. Cataract surgery may be performed for the following reasons:

E N D
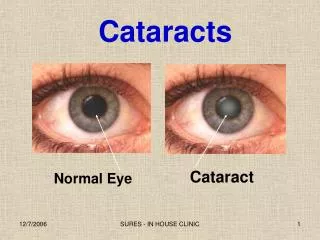
Management of senile cataract • Surgical by cataract extraction surgery
●Indications ● Techniques ● Complications
Indications Of Cataract Surgery • Cataract surgery may be performed for the following reasons: 1. To improve visual function (is by far the most frequent indication) 2. Medical indications: (a) As surgical therapy of glaucoma e.g. - Phacolytic glaucoma due to hypermature cataract and - Phacomorphic glaucoma or secondary ACG due to intumescent cataract. (b) To facilitate management of a posterior segment disease e.g. diabetic retinopathy.
■Techniques Of Cataract Surgery • Extracapsular cataract extraction (ECCE) 2. Phacoemulsification
1. Extracapsular cataract extraction (ECCE) □ Main Surgical Steps (surgical details are not required) • 1. Fornix-based conjunctival incision • 2. Limbal incision from 2 to 10 O'clock • 3. Anterior capsulotomy • 4. Delivery of lens nucleus • 5. Irrigation/Aspiration of lens cortex • 6. Healon (or any viscoelastic material) is injected into the AC to facilitate IOL implantation • 7. PC IOL is implanted in the capsular bag • 8. Irrigation/Aspiration of healon and any residual lens matter. • 9. Closure of the AC (limbal incision) • 10. Closure of the conjunctiva • 11. Subconjunctival injection of dexamethazone and antibiotic. • 12. Application of eye patch.
2. Phacoemulsification • Fragmentation • Irrigation • Aspiration
□ Main Surgical Steps (surgical details are not required) • 1. A small (1.5-3 mm) clear corneal or limbal incision • 2. Capsulotomy: continuous circular capsulorhexis (CCC) is made • 3. Emulsification of the nucleus involving 3 steps: a. sculpting of the central part of the nucleus b. Mobilizing the nucleus with a manipulating instrument c. Emulsifying of the remaining nucleus in a sequential manner. • 4. Aspiration of the remaining cortex • 5. injection of healon and foldable lens implantation • 6. Irrigation/Aspiration of healon • 7. The incision may or may not be sutured (according to its size) • 8. Subconjunctival injection of dexamethazone and antibiotic. • 9. Application of eye patch.
Complications of cataract surgery 1. Pre-operative (Anaesthetic) 2. Operative 3. Postoperative
1. Pre-operative (Anaesthetic) Complications • Retrobulbar hemorrhage • Inadvertent perforation of the globe • Penetration of optic nerve sheaths (subarachnoid space) respiratory distress • Intravascular injection of the anesthetic
2. Operative Complications 1. Rupture of posterior capsule predisposes to vitreous loss. 2. Vitreous loss predisposes to postoperative updrawn pupil, iris prolapse, vitreous touch, vitreous wick syndrome, uveitis, RD, and CME. 3. Massive suprachoroidal (expulsive) hemorrhage
3. Post-operative Complications • (a) Early • (b) Late
(A) Early Postoperative complications (Within the first few days of surgery) 1. Transient rise of IOP may be due to viscoelastic material (not entirely removed at end of surgery), or pupil block.
2. Iris prolapse predisposes to defective wound healing, postoperative astigmatism, uveitis, epithelial ingrowth, cystoid macular oedema, and bacterial endophthalmitis.
4. Wound leak resulting from inadequate wound suturing after ECCE.
(b) Late Postoperative complications • Suture-related problems e.g. Mechanical irritation, corneal vascularization, and GPC, and corneal 'suture' abscess.
2. Opacification of posterior capsule: esp. after ECCE. It is treated with YAG laser capsulotomy .
4. Bullous keratopathy due to endothelial decompensation (especially in eyes with AC IOL)
5. Epithelial ingrowth may cause severe refractory glaucoma.
6. Vitreous touch syndrome due to vitreous prolapse into AC (It was a common complication with ICCE, but uncommon with ECCE). 7. 'UGH' syndrome (uveitis, glaucoma, hyphema) in eyes with AC IOLs. Rare nowadays
8. Malposition of the IOL e.g. • 'Sunset syndrome' in which the PC IOL dislocates Inferiorly • 'Sunrise syndrome' in which the PC IOL dislocates superiorly.
9. RD especially in cases associated with PC rupture and vitreous loss.