Download
1 / 14
140 likes | 293 Views
Documenting Medical Necessity for Major Joint Replacements. James W. Cope, MD Jennifer Dupee, RN, JD. Improper Payments Elimination & Recovery Act of 2010 (IPERA). Requires Federal Agencies to: Identify programs that may be susceptible to significant improper payments;

E N D
Documenting Medical Necessity for Major Joint Replacements James W. Cope, MD Jennifer Dupee, RN, JD
Improper Payments Elimination & Recovery Act of 2010 (IPERA) Requires Federal Agencies to: • Identify programs that may be susceptible to significant improper payments; • Estimate the amount of improper payments in those programs; • Report the estimates to Congress and the public; and • Describe the actions the agency is taking to reduce improper payments in those programs.
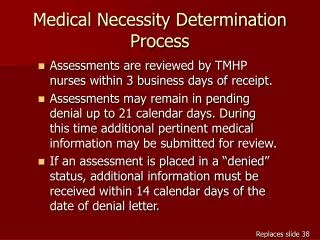
CMS Medical Review Entities *While these are the major review entities, CMS may implement additional special projects requiring medical review
Comprehensive Error Rate Testing (CERT) • Calculate the Medicare Fee-for-Service program improper payment rate • Claims are selected randomly from all claims submitted for payment during the reporting period (~ 50,000 claims) • Claim reviews are conducted by professional reviewers at the CERT Review Contractor • 85 RNs • 2 Medical Directors • 6 Coders
Comprehensive Error Rate Testing (CERT) • Determinations are made regarding whether the claim was paid properly under Medicare coverage, coding, and billing rules and error categories are assigned • Claims determined to be paid incorrectly are scored as errors and payments are adjusted • Improper payment rates are calculated and reported - www.cms.gov/cert
2011 CERT Findings • Rates • Adjusted Improper Payment Rate 8.6% ($28.8 Billion) • Downward adjustment applied for appeal results and receipt of supporting documentation received after the reporting cutoff date • Based on historical trends • Unadjusted Improper Payment Rate 9.9% ($33.3 Billion) • High-Error Claim Types: • Inpatient hospital short stays (medical necessity errors) • Physician services (coding errors) • DME (insufficient documentation errors)
Authority for Medical Review Social Security Act § 1862(a)(1)(A) (a) Notwithstanding any other provision of this title, no payment may be made under part A or part B for any expenses incurred for items or services— (1)(A) which, except for items and services described in a succeeding subparagraph, are not reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member
Authority for Medical Review 42 CFR § 424.5(a)(6) • As a basis for Medicare payment, the following conditions must be met: (6) Sufficient information. The provider, supplier, or beneficiary, as appropriate, must furnish to the intermediary or carrier sufficient information to determine whether payment is due and the amount of payment.
Documenting Medical Necessity for Major Joint Replacement (Hip and Knee) • MLN Matters SE1236: Published by CMS in September, 2012 • CERT & MACs found high improper payment rates among claims for hip and knee replacements • Described by CMS as “an educational guide to improve compliance with documentation requirements for major joint replacement surgery.” • To avoid denials, records should contain enough detailed information to support the medical necessity of the procedure. • “Painful DJD unresponsive to conservative treatment” is not enough.
History • Description of pain • ADL limitations • Safety • Contraindications to non-surgical treatments • Failed conservative treatments, e.g., • Meds (e.g., NSAIDs) • Weight loss • Physical Therapy • Intra-articular injections • Braces, orthotics or assistive devices.
Physical Examination • Deformity • Range of Motion • Crepitus • Effusions • Tenderness • Gait description
Investigations • Results of applicable investigations • Plain films • MRI
Clinical Judgment • Reasons for deviating from a stepped-care approach • Intolerant of NSAIDs • Refused injections • Joint damage too severe to respond (e.g., AVN femoral head) Must be clearly documented