Download
1 / 32
330 likes | 500 Views
The digestive system & Liver function tests. I-The digestive system. Digestion. Digestion is the mechanical and chemical breaking down of food into smaller components that can be absorbed into a blood stream

E N D
Digestion • Digestion is the mechanical and chemical breaking down of food into smaller components that can be absorbed into a blood stream • Digestion is a form of catabolism: a break-down of larger food molecules to smaller ones.
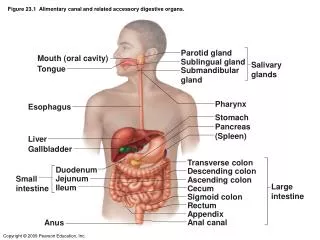
Digestive system • In mammals, food enters the mouth, being chewed by teeth, with chemical processing beginning with chemicals in the saliva from the salivary glands. • Then it travels down the esophagus into the stomach, where hydrochloric acid kills most contaminating microorganisms and begins mechanical break down of some food (e.g., denaturation of protein), and chemical alteration of some. • After some time (typically an hour or two in humans, the results go through the small intestine, through the large intestine, and are excreted during defecation.
-stomy • This means a mouth or opening. Usually a stoma is formed by surgery • e.g. a colostomy is an opening or the formation of an opening into the colon. • This word component is also used in anastomosis, an operation to form an opening/communication between two parts. • A stoma can be temporary or permanent. -tomy • Means an incision as at the beginning of an operation.
Related conditions Gastritis inflammation of stomach GastroenteritisInflammation of the stomach and intestine Gastrectomy Excision of stomach Hepatitis inflammation of liver Hepatoma tumor of liver Laparotomy cutting into the abdomen Laparoscopy visual exam of the abdomen
Related conditions Cholelithotomy removal of gall stones Cholelithiasis gall stones causing symptoms Cholecystitis inflammation of gallbladder Cholecystectomy removal of gallbladder Emetic stimulating vomiting Antiemetic stopping vomiting Melanocyte cells produce melanin Melanoma Melanin producing tumor
Related conditions • Lymphangiectasis Dialation of a lymph vessel • Dyspepsia Difficult digestion • Dysphagia Difficulty in swallowing • SplenorrhagiaBursting forth of blood from the spleen • Menorrhagia Heavy menstrual discharge • Sialolithiasis Salivary stones • Hematemesis Vomiting of blood
Related conditions • Esophageal atresia no opening of the esophaagus at birth • Cecostomy new opening of the first part of the colon to the outside • Jejunoje/junostomy New opening between two parts of the jejunum • Pyloric Stenosis Narrowing of the opening between the stomach and intestine • Hemoptysis Spitting up blood from the respiratory tract and lungs.
Endoscopy Use of a fiberoptic endoscope for direct visual examination. GI studies include • Esophagogastroduodenoscopy • Proctosigmoidoscopy (rectum and distal colon) • Colonoscopy (all regions of the colon) • Gastroscopy(stomach)
Colic • Acute abdominal pain, such as biliary colic caused by gallstones in the bile ducts • Paracentesis • Collection of peritoneal fluid • Cirrhosis • Chronic liver disease with degeneration of liver tissue.
Bilirubin • A pigment released in the breakdown of hemoglobin from red blood cells; mainly excreted by the liver in bile • Icterus • Jaundice • Jaundice • A yellowish color of the skin, mucous membranes, and whites of the eye caused by bile pigments in the blood (from French jaune meaning“yellow”). The main pigment is bilirubin.
peptic ulcer • A lesion in the mucous membrane of the esophagus, stomach, or duodenum caused by the action of gastric juice • ulcerative colitis • Chronic ulceration of the colon of unknown cause
Anorexia • Loss of appetite. Anorexia nervosa is a psychologically induced refusal or inability to eat • Constipation • Infrequency or difficulty in defecation and the passage of hard, dry feces.
Liver • The liver is the largest organ in the body • It consists of two main lobes that together weigh from 1400 to 1600 g in the normal adult • It is reddish brown in color and has a rich blood supply 1500 ml/min from two major vessels, the hepatic artery and the portal vein
Structural Unit • The lobule which measures 1-2 mm in diameter, forms the structural unit of the liver. • It is composed of cords of liver cells (hepatocytes) radiating from a central vein. • Between the cords of the liver cells are vascular spaces, called sinusoids, that are lined by endothelial cells and Kupffer’s cells • The Kupffer’s cells are phagocytic macrophages capable of ingesting bacteria or other foreign material from the blood that flows through the sinusoids
Physiology The liver has a central role in the metabolism of carbohydrates, lipids, proteins, vitamins and hormones, as well as a role as a storage and excretory organ. It has an important role in detoxification and drug metabolism.
Liver Function Tests • The routine liver function tests include the measurement of : • Total , direct and indirect bilirubin • Total proteins and albumin • Liver enzymes include : • ALT ( Alanine transaminase ) • AST ( Aspartate transaminase ) • AlP ( Alkaline phosphatase ) • GGT ( - Glutamyl transferase )
Except for the screening of healthy people (for insurance examinations or occupational medicine), liver function tests are usually employed in patients to: • Confirm a clinical suspicion of the presence of liver disease. • Give an idea about the severity and prognosis of the liver disease. • Follow up the disease and evaluate therapy. • Arrive at a differential diagnosis (e.g. cholestatic vs • hepatocellular liver disease).
Bilirubin Metabolism • It is mainly in reticulo-endothelial system (liver, spleen and bone marrow), Liver and intestine • 80% of bilirubin formed from heme each day arise from red blood cells. • Iron is removed from the heme molecule and the porphyrin ring is opened to form bilirubin. • Total serum bilirubin is equal to the sum of the two types of bilirubin • Direct (conjugated) bilirubin. • Indirect (unconjugated) bilirubin
Jaundice may be classified into: • Pre-hepatic Jaundice: • The production rate of bilirubin is increased, exceeding the excretory capacity of the liver. Overproduction of bilirubin occurs in all forms of hemolytic anemia, less commonly, in conditions where there is much ineffective erythropoiesis (e.g. pernicious anemia). • There is increase in plasma indirect (unconjugated) bilirubin. • Bilirubin is not excreted in urine. • Urinary urobilinogen concentration is increased.
2) Hepatocellular Jaundice: • Hepatocellular damage due to viral hepatitis or toxins may interfere with the uptake of bilirubin, or with its conjugation or with secretion of conjugated bilirubin into bile. • Both indirect and direct hyperbilirubinemia may occur in hepatocellular jaundice. • Bilirubin and excess urobilinogen are found in urine.
3)Obstructive (Cholestatic) Jaundice: • It is due to impaction of gallstones in the common bile duct or carcinoma of the head of pancreas or of the biliary tree. • Jaundice is due to conjugated (direct) bilirubin. • Bilirubin is detected in urine.
Congenital Hyperbilirubinemias: They are all due to inherited defects in the mechanism of bilirubin transport.
Albumin Albumin has a long half-life of 20 days and levels fall slowly if no synthesis occur. Thus, serum albumin is usually normal in acute hepatitis. However, in chronic liver diseases such as cirrhosis, impaired synthesis may lead to low serum levels. Serum albumin levels may be low due to loss into urine, gut or into a third compartment (ascitis).
Serum Enzymes in liver disease • a) Aminotransferases (ALT & AST): • Aminotransferases are involved in amino acid metabolism. • AST occurs in both the cytosol and mitochondria of cells while ALT is a cytosolic enzyme. • Increased amounts of both transaminases leak from inflamed or damaged hepatocytes due to acute or chronic hepatitis. • ALT is more specific for liver disease than AST .
b) Alkaline Phosphatase (ALP): • Originates from the liver, bone (reflecting osteoblastic activity) and the placenta. • Levels of ALP increase in cholestasis, mainly because of increased synthesis.
c) - Glutamyl transferase (GGT): Increased serum levels of GGT are found in both hepatocellular and cholestatic disease. Higher levels are found in cholestasis. Increased synthesis of GGT is induced by excessive ethanol intake.
N.B. Hepatic Enzymes: • ALT and AST levels are raised mainly in hepatocellular disease. • AlP level is raised mainly in obstructive disease. • The increased in serum GGT levels are modest in hepatocellular disease and marked in obstructive disease.