Download
1 / 1
10 likes | 155 Views
Bevacizumab (B) (5mg/Kg) in combination with Cisplatin (C) and Docetaxel (D) administered every 2 weeks in patients (p) with advanced non-squamous Non-Small Cell Lung Cancer (nsNSCLC) : GGCP047/10 study

E N D
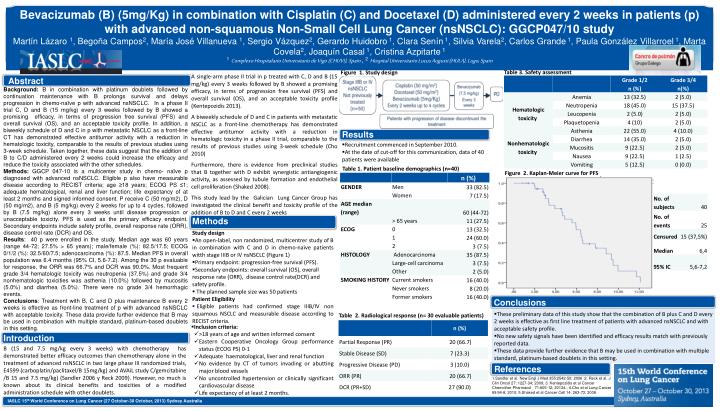
Bevacizumab (B) (5mg/Kg) in combination with Cisplatin (C) and Docetaxel (D) administered every 2 weeks in patients (p) with advanced non-squamous Non-Small Cell Lung Cancer (nsNSCLC): GGCP047/10 study Martín Lázaro 1, Begoña Campos2, María José Villanueva 1, Sergio Vázquez2, Gerardo Huidobro 1, Clara Senín 1, Silvia Varela2, Carlos Grande 1, Paula González Villarroel 1, Marta Covela2, Joaquín Casal 1, Cristina Azpitarte 1 1Complexo Hospitalario Universitario de Vigo (CHUVI), Spain , 2Hospital Universitario Lucus Augusti (HULA), Lugo, Spain Figure 1. Study design Table 3. Safety assessment A single-arm phase II trial in p treated with C, D and B (15 mg/kg) every 3 weeks followed by B showed a promising efficacy, in terms of progression free survival (PFS) and overall survival (OS), and an acceptable toxicity profile (Kentepozidis 2013). A biweekly schedule of D and C in patients with metastatic NSCLC as a front-line chemotherapy has demonstrated effective antitumor activity with a reduction in hematologic toxicity in a phase II trial, comparable to the results of previous studies using 3-week schedule (Cho 2010) Furthermore, there is evidence from preclinical studies that B together with D exhibit synergistic antiangiogenic activity, as assessed by tubule formation and endothelial cell proliferation (Shaked 2008). This study lead by the Galician Lung Cancer Group has investigated the clinical benefit and toxicity profile of the addition of B to D and C every 2 weeks Background: B in combination with platinum doublets followed by continuation maintenance with B prolongs survival and delays progression in chemo-naïve p with advanced nsNSCLC. In a phase II trial C, D and B (15 mg/kg) every 3 weeks followed by B showed a promising efficacy, in terms of progression free survival (PFS) and overall survival (OS), and an acceptable toxicity profile. In addition, a biweekly schedule of D and C in p with metastatic NSCLC as a front-line CT has demonstrated effective antitumor activity with a reduction in hematologic toxicity, comparable to the results of previous studies using 3-week schedule. Taken together, these data suggest that the addition of B to C/D administered every 2 weeks could increase the efficacy and reduce the toxicity associated with the other schedules. Methods: GGCP 047-10 is a multicenter study in chemo- naïve p diagnosed with advanced nsNSCLC. Eligible p also have measurable disease according to RECIST criteria; age ≥18 years; ECOG PS ≤1; adequate hematological, renal and liver function; life expectancy of at least 2 months and signed informed consent. P receive C (50 mg/m2), D (50 mg/m2), and B (5 mg/kg) every 2 weeks for up to 4 cycles, followed by B (7.5 mg/kg) alone every 3 weeks until disease progression or unacceptable toxicity. PFS is used as the primary efficacy endpoint. Secondary endpoints include safety profile, overall response rate (ORR), disease control rate (DCR) and OS. Results: 40 p were enrolled in the study. Median age was 60 years (range 44-72; 27.5% > 65 years); male/female (%): 82.5/17.5; ECOG 0/1/2 (%): 32.5/60/7.5; adenocarcinoma (%): 87.5. Median PFS in overall population was 6.4 months (95% CI, 5.6-7.2). Among the 30 p evaluable for response, the ORR was 66.7% and DCR was 90.0%. Most frequent grade 3/4 hematologic toxicity was neutropenia (37.5%) and grade 3/4 nonhematologic toxicities was asthenia (10.0%) followed by mucositis (5.0%) and diarrhea (5.0%). There were no grade 3/4 hemorrhagic events. Conclusions: Treatment with B, C and D plus maintenance B every 2 weeks is effective as front-line treatment of p with advanced nsNSCLC with acceptable toxicity. These data provide further evidence that B may be used in combination with multiple standard, platinum-based doublets in this setting. Abstract • Recruitment commenced in September 2010. • At the date of cut-off for this communication, data of 40 patients were available Table 1. Patient baseline demographics (n=40) Figure 2. Kaplan-Meier curve for PFS • Study design • An open-label, non randomized, multicentrer study of B in combination with C and D in chemo-naïve patients witth stage IIIB or IV nsNSCLC (Figure 1) • Primary endpoint: progression-free survival (PFS). • Secondary endpoints: overall survival (OS), overall response rate (ORR), disease control rate(DCR) and safety profile. • The planned sample size was 50 patients • Patient Eligibility • Eligible patients had confirmed stage IIIB/IV non squamous NSCLC and measurable disease according to RECIST criteria. Results Conclusions Methods Table 2. Radiological response (n= 30 evaluable patients) • These preliminary data of this study show that the combination of B plus C and D every 2 weeks is effective as first line treatment of patients with advanced nsNSCLC and with acceptable safety profile. • No new safety signals have been identified and efficacy results match with previously reported data. • These data provide further evidence that B may be used in combination with multiple standard, platinum-based doublets in this setting. • Inclusion criteria: • >18 years of age and written informed consent • Eastern Cooperative Oncology Group performance status (ECOG PS) 0-1 • Adequate haematological, liver and renal function • No evidence by CT of tumors invading or abutting major blood vessels • No uncontrolled hypertension or clinically significant cardiovascular disease • Life expectancy of at least 2 months. References B (15 and 7.5 mg/kg every 3 weeks) with chemotherapy has demonstrated better efficacy outcomes than chemotherapy alone in the treatment of advanced nsNSCLC in two large phase III randomized trials, E4599 (carboplatin/paclitaxel/B 15mg/kg) and AVAiL study C/gemcitabine /B 15 and 7.5 mg/kg) (Sandler 2006 y Reck 2009). However, no much is known about its clinical benefits and toxicities of a modified administration schedule with other doublets. Introduction 1.Sandler et al. New Engl J Med 355:2542-50; 2006 ;2. Reck et al. J Clin Oncol 27: 1227-34; 2009; 3. Kentepozidis et al Cancer Chemother Pharmacol 71:605-12; 20134.; 4.Cho et al Lung Cancer 69:94-8; 2010; 5.Shaked et al Cancer Cell 14: 263-73; 2008 IASLC 15th World Conference on Lung Cancer (27 October-30 October, 2013) Sydney Australia






