Download
1 / 50
590 likes | 904 Views
Proteinuria and Hypertension in Kidney Transplant. Chih-Kang Chiang, MD, PhD Department of Diagnostics & Theraputics and Internal Medicine, National Taiwan University Hospital Nov.24, 2006. Conceptual model for stages in the initiation and progression of CKD, and therapeutic interventions.

E N D
Proteinuria and Hypertension in Kidney Transplant Chih-Kang Chiang, MD, PhD Department of Diagnostics & Theraputics and Internal Medicine, National Taiwan University Hospital Nov.24, 2006
Conceptual model for stages in the initiation and progression of CKD, and therapeutic interventions.
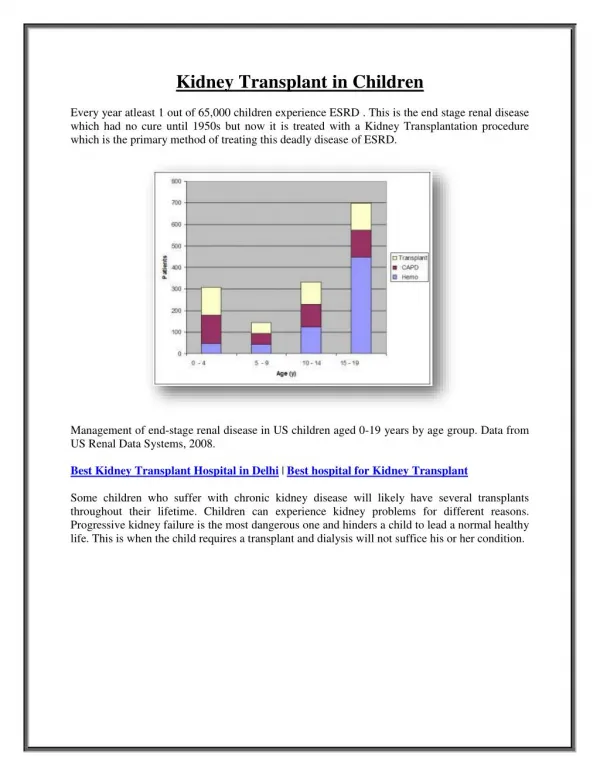
Stage and Prevalence of CKD • NHANES III (19881994) and USRDS (1998)
Chronic Kidney Disease (CKD) Staging V I IV II III
General approach to hypertension and use of antihypertensive agents in CKD.
Classification of CKD by Diagnosis and prevalence of Kidney Failure
Albuminuria as a risk factor for CVD in individuals without diabetes. (ref 8)
Hypothesized Pathogenic Mechanisms of High Blood Pressure in CKD Ref 22
CVD Mortality in Kidney Transplant Patients vs. General Population
Traditional vs. CKD-Related Factors Related to an Increased Risk of CVD ref 25.27
Classification of Hypertension JNC VII
Risk factors for kidneydisease progression related to hypertension.
Effect of antihypertensive drugs on systemicand glomerular pressure.
Mechanisms of antihypertensive agentsto slow progression of CKD
Strategies and Therapeutic Targets for Anti-HTN Agents in CKD
Hypertension and Kidney Transplant • Hypertension occurs in up to 80% of kidney transplant recipients. • In the recently completed 5-year cadaveric kidney transplant trial: Antihypertensive therapy was used • in 81% of tacrolimus treated recipients • in 90% of cyclosporine-treated recipients
Hypertension and Graft Survival • Collaborative Transplant Study
Pharmacological Therapy:Kidney Disease in the Kidney Transplant Recipient • Most kidney transplant recipients have CKD and hypertension. High blood pressure in kidney transplant recipients is a risk factor for faster progression of CKD and development of CVD. • 10.1 The target blood pressure in kidney transplant recipients should be <130/80 mm Hg (see Guideline 7) (Table 119). • 10.2 Patients with CKD in the kidney transplant should be treated with any of the following to reach the target blood pressure: CCB, diuretics, ACE inhibitor, ARB, or beta-blocker (Table 119).
CKD in Kidney Transplant Recipients • Most kidney transplant recipients have CKD • Either kidney damage or • GFR 60 mL/min/1.73 m2 for 3 months • GFR is lower in individuals • A solitary kidney • Toxicity from immunosuppressive agents • cyclosporine • tacrolimus • Rejection
Stages and Clinical Features of Diseases in the Kidney Transplant Recipients
Drug intervention in Kidney Transplant Recipients (I) • The available data on treatment of posttransplant hypertension are insufficient to recommend any class of antihypertensive agents as preferred agents for long-term therapy to slow the progression of kidney disease (Moderately Strong).
Drug intervention in Kidney Transplant Recipients (II) • Dihydropyridine(DHP) calcium-channel blockers are associated with higher GFR after transplantation in short-term studies (Strong). • ameliorating vasoconstriction of the afferent arteriole induced by calcineurin inhibitors (cyclosporine and tacrolimus). • Fewer DGF and acute rejection episodes, and possibly also a better long-term graft function.
Drug intervention in Kidney Transplant Recipients (III) • DHP-CCB (nifedipine, amlodipine,and isradipine) • CYP3A4 competition substrate • Non-DHP-CCB (verapamil and diltiazem) • CYP3A4 inhibitor
Drug intervention in Kidney Transplant Recipients (IV) • ACEI/ARB: (hyperkalemia, anemia, ARF) • Maybe beneficial effects on the progression of kidney disease, as in diabetic and nondiabetic kidney disease • ischemic heart disease (IHD) • TGFβ DGF • Lorenz et al draws 2 important conclusions: • (1) the early use of ACEIs/ARBs is safe with no compromise of graft function, and • (2) patients with DGF might benefit from blockade of the RAS system by shortening the time to graft recovery.
Drug intervention in Kidney Transplant Recipients (V) • β-blockers: • an adjunct agent for control of blood pressure (High CVD in transplant receipient) • ischemic heart disease (IHD) • Diuretics • hypertension in cyclosporine treated patients may be sodium-dependent
Kidney transplant recipients have a high risk of CVD (Strong). • Hypertension is a risk factor for CVD in kidney transplant recipients (Moderately Strong).
High blood pressure is a risk factor for faster progression of kidney disease in kidney transplant recipients (Moderately Strong). • Proteinuria after transplantation is a risk factor for graft loss and death (Moderately Strong).
Hypertension and Anti-HTN agents in Kidney Disease in the Kidney Transplant Recipient
Summary of Recommendations in Kidney Transplant Recipients (I)
Summary of Recommendations in Kidney Transplant Recipients (II)
Beta-blocker use was associated with higher UA level (8.92.0 vs. 8.02.0 mg/dL, [0.530.12 vs. 0.480.12 mmol/L], P<0.009).
URICOSURIC EFFECT OF LOSARTAN IN PATIENTS WITH RENAL TRANSPLANTS Losartan is a potent inhibitor of the urate/anion exchanger in human proximal tubules Kamper et al. Transplantation, 72(4), 2001.671-674