Download
1 / 34
340 likes | 446 Views
Obesity Trends Among U.S. Adults between 1985 and 2006. Definitions: Obesity: Having a very high amount of body fat in relation to lean body mass, or Body Mass Index (BMI) of 30 or higher.

E N D
Obesity Trends Among U.S. Adults between 1985 and 2006 • Definitions: • Obesity: Having a very high amount of body fat in relation to lean body mass, or Body Mass Index (BMI) of 30 or higher. • Body Mass Index (BMI): A measure of an adult’s weight in relation to his or her height, specifically the adult’s weight in kilograms divided by the square of his or her height in meters. • Adult BMI calculators are available free on the internet.
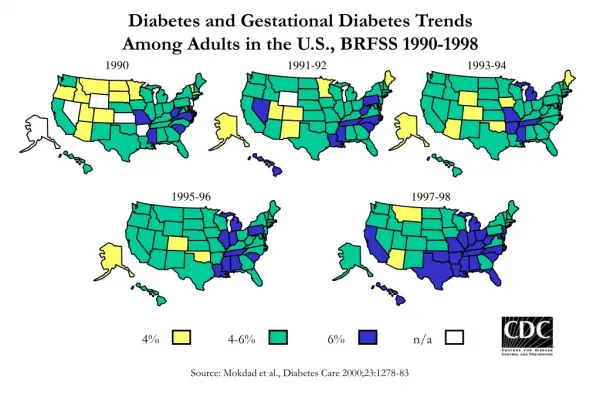
Obesity Trends Among U.S. Adults between 1985 and 2006 • Source of the data: • The data shown in these maps were collected through CDC’s Behavioral Risk Factor Surveillance System (BRFSS). Each year, state health departments use standard procedures to collect data through a series of monthly telephone interviews with U.S. adults. • Prevalence estimates generated for the maps may vary slightly from those generated for the states by BRFSS (http://aps.nccd.cdc.gov/brfss) as slightly different analytic methods are used.
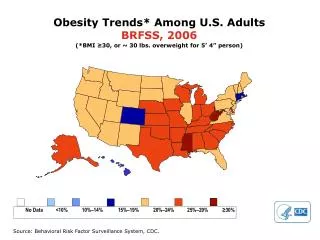
In 1990, among states participating in the Behavioral Risk Factor Surveillance System, 10 states had a prevalence of obesity less than 10% and no states had prevalence equal to or greater than 15%. • By 1998, no state had prevalence less than 10%, seven states had a prevalence of obesity between 20-24%, and no state had prevalence equal to or greater than 25%. • In 2006, only four states had a prevalence of obesity less than 20%. Twenty-two states had a prevalence equal or greater than 25%; Two of these states (Mississippi and West Virginia) had a prevalence of obesity equal to or greater than 30%.
Obesity Trends* Among U.S. AdultsBRFSS,1990, 1998, 2006 (*BMI 30, or about 30 lbs. overweight for 5’4” person) 1998 1990 2006 No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
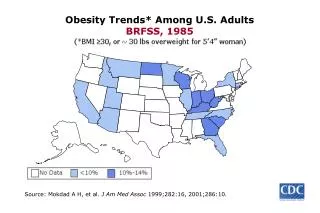
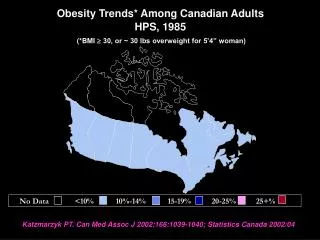
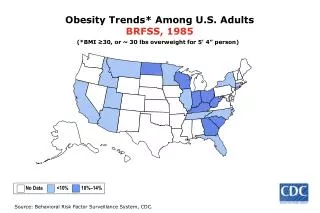
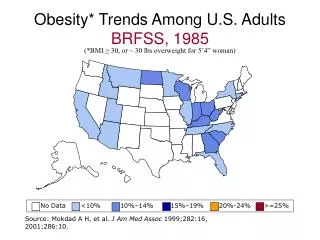
Obesity Trends* Among U.S. AdultsBRFSS, 1985 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14%
Obesity Trends* Among U.S. AdultsBRFSS, 1986 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14%
Obesity Trends* Among U.S. AdultsBRFSS, 1987 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14%
Obesity Trends* Among U.S. AdultsBRFSS, 1988 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14%
Obesity Trends* Among U.S. AdultsBRFSS, 1989 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14%
Obesity Trends* Among U.S. AdultsBRFSS, 1990 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14%
Obesity Trends* Among U.S. AdultsBRFSS, 1991 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19%
Obesity Trends* Among U.S. AdultsBRFSS, 1992 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19%
Obesity Trends* Among U.S. AdultsBRFSS, 1993 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19%
Obesity Trends* Among U.S. AdultsBRFSS, 1994 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19%
Obesity Trends* Among U.S. AdultsBRFSS, 1995 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19%
Obesity Trends* Among U.S. AdultsBRFSS, 1996 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19%
Obesity Trends* Among U.S. AdultsBRFSS, 1997 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% ≥20%
Obesity Trends* Among U.S. AdultsBRFSS, 1998 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% ≥20%
Obesity Trends* Among U.S. AdultsBRFSS, 1999 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% ≥20%
Obesity Trends* Among U.S. AdultsBRFSS, 2000 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% ≥20%
Obesity Trends* Among U.S. AdultsBRFSS, 2001 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% ≥25%
Obesity Trends* Among U.S. AdultsBRFSS, 2002 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% ≥25%
Obesity Trends* Among U.S. AdultsBRFSS, 2003 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% ≥25%
Obesity Trends* Among U.S. AdultsBRFSS, 2004 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% ≥25%
Obesity Trends* Among U.S. AdultsBRFSS, 2005 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
Obesity Trends* Among U.S. AdultsBRFSS, 2006 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
Health Consequences Overweight and obese individuals are at increased risk for many diseases and health conditions, including the following: • Hypertension (high blood pressure) • Osteoarthritis (a degeneration of cartilage and its underlying bone within a joint) • Dyslipidemia (for example, high total cholesterol or high levels of triglycerides) • Type 2 diabetes • Coronary heart disease • Stroke • Gallbladder disease • Sleep apnea and respiratory problems • Some cancers (endometrial, breast, and colon)
Economic Consequences Overweight and obesity and their associated health problems have a significant economic impact on the U.S. health care system (USDHHS, 2001). Medical costs associated with overweight and obesity may involve direct and indirect costs (Wolf and Colditz, 1998; Wolf, 1998). Direct medical costs may include preventive, diagnostic, and treatment services related to obesity. Indirect costs relate to morbidity and mortality costs. Morbidity costs are defined as the value of income lost from decreased productivity, restricted activity, absenteeism, and bed days. Mortality costs are the value of future income lost by premature death.
Economic Consequences • In 1995, the total (direct and indirect) costs attributable to obesity amounted to an estimated $99 billion. In 2000, the total cost of obesity was estimated to be $117 billion ($61 billion direct and $56 billion indirect). Most of the cost associated with obesity is due to type 2 diabetes, coronary heart disease, and hypertension.
What are some suggestions for losing weight? • Most experts recommend that someone attempting to lose a large amount of weight consult with a personal physician or health care professional before beginning a weight-loss program. The Surgeon General’s Healthy Weight Advice for Consumers makes the following general recommendations: • Aim for a healthy weight. People who need to lose weight should do so gradually, at a rate of one-half to two pounds per week. • Be active. The safest and most effective way to lose weight is to reduce calories and increase physical activity. • Eat well. Select sensible portion sizes and follow the Dietary Guidelines for Americans.
How can physical activity help prevent overweight and obesity? • Physical activity, along with a healthy diet, plays an important role in the prevention of overweight and obesity (USDHHS, 2001). In order to maintain a stable weight, a person needs to expend the same amount of calories as he or she consumes. • Although the body burns calories for everyday functions such as breathing, digestion, and routine daily activities, many people consume more calories than they need for these functions each day. A good way to burn off extra calories and prevent weight gain is to engage in regular physical activity beyond routine activities.
How can physical activity help prevent overweight and obesity? • The Dietary Guidelines for Americans 2005 offers the following example of the balance between consuming and using calories: • If you eat 100 more food calories a day than you burn, you’ll gain about 1 pound in a month. That’s about 10 pounds in a year. The bottom line is that to lose weight, it’s important to reduce calories and increase physical activity.
For more information about losing weight, visit • Dietary Guidelines for Americans 2005Department of Health and Human Services (HHS) and the Department of Agriculture (USDA) • Aim for a Healthy WeightNational Institutes of Health (NIH), National Heart, Lung, and Blood Institute (NHLBI) • Weight-control Information Network: PublicationsNational Institutes of Health (NIH), National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), Weight-control Information Network • The Surgeon General's Call to Action to Prevent and Decrease Overweight and Obesity: Surgeon General’s Healthy Weight Advice for Consumers
Citations • BRFSS, Behavioral Risk Factor Surveillance System http: //www.cdc.gov/brfss/ • Mokdad AH, et al. The spread of the obesity epidemic in the United States, 1991—1998 JAMA 1999; 282:16:1519–1522. • Mokdad AH, et al. The continuing epidemics of obesity and diabetes in the United States. JAMA. 2001; 286:10:1519–22. • Mokdad AH, et al. Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA 2003: 289:1: 76–79 • CDC. State-Specific Prevalence of Obesity Among Adults — United States, 2005; MMWR 2006; 55(36);985–988