Download
1 / 1
10 likes | 137 Views
2006 AAO Annual Meeting. Ocular radiation hazard of medical practitioners involving radiation exposure. Andrew K . C . L AM 1 , PhD, FAAO; Karl KL FUNG 2 , MSc, PhD; Suk-tak CHAN 2 , PhD.

E N D
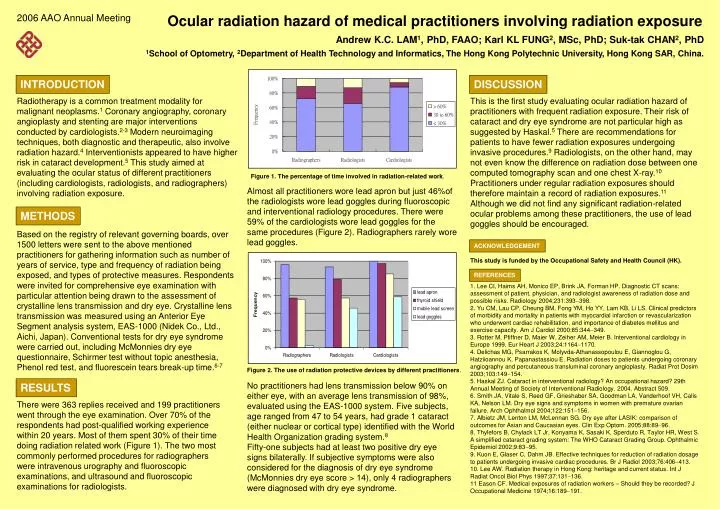
2006 AAO Annual Meeting Ocular radiation hazard of medical practitioners involving radiation exposure Andrew K.C. LAM1, PhD, FAAO; Karl KL FUNG2, MSc, PhD; Suk-tak CHAN2, PhD 1School of Optometry, 2Department of Health Technology and Informatics, The Hong Kong Polytechnic University, Hong Kong SAR, China. INTRODUCTION DISCUSSION Radiotherapy is a common treatment modality for malignant neoplasms.1 Coronary angiography, coronary angioplasty and stenting are major interventions conducted by cardiologists.2-3 Modern neuroimaging techniques, both diagnostic and therapeutic, also involve radiation hazard.4Interventionists appeared to have higher risk in cataract development.5This study aimed at evaluating the ocular status of different practitioners (including cardiologists, radiologists, and radiographers) involving radiation exposure. Based on the registry of relevant governing boards, over 1500 letters were sent to the above mentioned practitioners for gathering information such as number of years of service, type and frequency of radiation being exposed, and types of protective measures. Respondents were invited for comprehensive eye examination with particular attention being drawn to the assessment of crystalline lens transmission and dry eye. Crystalline lens transmission was measured using an Anterior Eye Segment analysis system, EAS-1000 (Nidek Co., Ltd., Aichi, Japan). Conventional tests for dry eye syndrome were carried out, including McMonnies dry eye questionnaire, Schirmer test without topic anesthesia, Phenol red test, and fluorescein tears break-up time.6-7 This is the first study evaluating ocular radiation hazard of practitioners with frequent radiation exposure. Their risk of cataract and dry eye syndrome are not particular high as suggested by Haskal.5 There are recommendations for patients to have fewer radiation exposures undergoing invasive procedures.9 Radiologists, on the other hand, may not even know the difference on radiation dose between one computed tomography scan and one chest X-ray.10 Practitioners under regular radiation exposures should therefore maintain a record of radiation exposures.11 Although we did not find any significant radiation-related ocular problems among these practitioners, the use of lead goggles should be encouraged. Almost all practitioners wore lead apron but just 46%of the radiologists wore lead goggles during fluoroscopic and interventional radiology procedures. There were 59% of the cardiologists wore lead goggles for the same procedures (Figure 2). Radiographers rarely wore lead goggles. No practitioners had lens transmission below 90% on either eye, with an average lens transmission of 98%, evaluated using the EAS-1000 system. Five subjects, age ranged from 47 to 54 years, had grade 1 cataract (either nuclear or cortical type) identified with the World Health Organization grading system.8 Fifty-one subjects had at least two positive dry eye signs bilaterally. If subjective symptoms were also considered for the diagnosis of dry eye syndrome (McMonnies dry eye score > 14), only 4 radiographers were diagnosed with dry eye syndrome. Figure 1. The percentage of time involved in radiation-related work. METHODS ACKNOWLEDGEMENT This study is funded by the Occupational Safety and Health Council (HK). REFERENCES 1. Lee CI, Haims AH, Monico EP, Brink JA, Forman HP. Diagnostic CT scans: assessment of patient, physician, and radiologist awareness of radiation dose and possible risks. Radiology 2004;231:393398. 2. Yu CM, Lau CP, Cheung BM, Fong YM, Ho YY, Lam KB, Li LS. Clinical predictors of morbidity and mortality in patients with myocardial infarction or revascularization who underwent cardiac rehabilitation, and importance of diabetes mellitus and exercise capacity. Am J Cardiol 2000;85:344349. 3. Rotter M, Pfiffner D, Maier W, Zeiher AM, Meier B. Interventional cardiology in Europe 1999. Eur Heart J 2003;24:11641170. 4. Delichas MG, Psarrakos K, Molyvda-Athanassopoulou E, Giannoglou G, Hatziioannou K, Papanastassiou E. Radiation doses to patients undergoing coronary angiography and percutaneous transluminal coronary angioplasty. Radiat Prot Dosim 2003;103:149154. 5. Haskal ZJ. Cataract in interventional radiology? An occupational hazard? 29th Annual Meeting of Society of Interventional Radiology. 2004. Abstract 509. 6. Smith JA, Vitale S, Reed GF, Grieshaber SA, Goodman LA, Vanderhoof VH, Calis KA, Nelson LM. Dry eye signs and symptoms in women with premature ovarian failure. Arch Ophthalmol 2004;122:151156. 7. Albietz JM, Lenton LM, McLennan SG. Dry eye after LASIK: comparison of outcomes for Asian and Caucasian eyes. Clin Exp Optom. 2005;88:8996. 8. Thylefors B, Chylack LT Jr, Konyama K, Sasaki K, Sperduto R, Taylor HR, West S. A simplified cataract grading system: The WHO Cataract Grading Group. Ophthalmic Epidemiol 2002;9:8395. 9. Kuon E, Glaser C, Dahm JB. Effective techniques for reduction of radiation dosage to patients undergoing invasive cardiac procedures. Br J Radiol 2003;76:406413. 10. Lee AW. Radiation therapy in Hong Kong: heritage and current status. Int J Radiat Oncol Biol Phys 1997;37:131136. 11 Eason CF. Medical exposures of radiation workers – Should they be recorded? J Occupational Medicine 1974;16:189191. Figure 2. The use of radiation protective devices by different practitioners. RESULTS There were 363 replies received and 199 practitioners went through the eye examination. Over 70% of the respondents had post-qualified working experience within 20 years. Most of them spent 30% of their time doing radiation related work (Figure 1). The two most commonly performed procedures for radiographers were intravenous urography and fluoroscopic examinations, and ultrasound and fluoroscopic examinations for radiologists.